Inquiries by Email
Inquiries by Email
Stem cell therapy for Parkinson’s disease in Japan in 2026 centers on Amchepry’s iPS-derived dopaminergic cell transplantation and intravenous adipose-derived MSC infusion, set against the long-established deep brain stimulation (DBS) standard.
Below: Amchepry’s MHLW approval and ¥55.3M reimbursement structure, where DBS fits for advanced motor fluctuations, and what realistic 2026 access looks like for non-Japanese patients.
Cell Grand Clinic in Osaka provides up to 200 million autologous ADSCs from your own minimal fat tissue, cultured over 7 weeks and delivered intravenously as supportive care for Parkinson’s-associated frailty — never donor cells.
MHLW Type 2 certified · NIH-trained physician · 3,000+ ADSC cases across ~20 countries · written second-opinion case review.
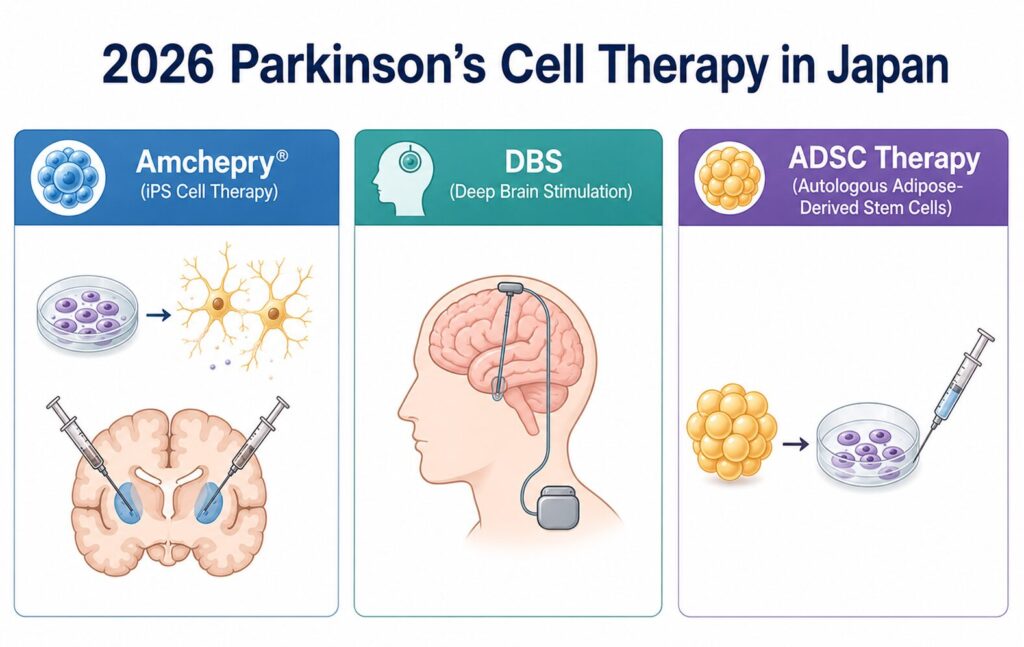
Amchepry (Sumitomo Pharma, Japan) — the world’s first iPS-derived cell therapy for Parkinson’s disease — received conditional, time-limited approval from the Japanese Ministry of Health, Labour and Welfare (MHLW) in March 2026 and entered national health insurance reimbursement on May 20, 2026 at ¥55.3 million (≈ $350,000 USD) per patient. International patients reading “Japan’s stem cell breakthrough” headlines often ask three questions: Can I get it? What’s the alternative? And what does a regenerative-medicine physician actually recommend? This 2026 guide, written by an MHLW-certified physician with over 3,000 adipose-derived stem cell (ADSC) cases across roughly 20 countries, focuses on the three options available in Japan today — Amchepry, deep brain stimulation (DBS), and mesenchymal stem cell (MSC/ADSC) therapy — including the practical access reality for non-Japanese patients, and where realistic, honest supportive care fits in.
- Japan’s breakthrough — what changed for Parkinson’s in 2026?
- How Amchepry works — iPS-derived dopaminergic cells delivered by stereotactic brain surgery
- Can international patients get Amchepry in Japan? The honest answer
- Deep brain stimulation (DBS) for Parkinson’s — what it does, what it doesn’t
- Mesenchymal stem cell (MSC/ADSC) therapy for Parkinson’s — mechanism, evidence, what’s realistic
- Side-by-side: Amchepry vs DBS vs MSC/ADSC
- What the clinical evidence actually says — trials, meta-analyses, and the honest limits
- What Cell Grand Clinic can — and cannot — offer Parkinson’s patients
- Considering supportive care alongside your standard Parkinson’s treatment?
- Frequently asked questions
- Summary — hope, honesty, and what comes next
- References
Japan’s breakthrough — what changed for Parkinson’s in 2026?
Direct AnswerIn 2026, Japan became the first country to approve and reimburse an iPS-derived cell therapy for Parkinson’s disease. Amchepry (Sumitomo Pharma), an allogeneic iPS-derived dopaminergic progenitor product developed at Kyoto University’s CiRA, received conditional MHLW approval in March 2026 and entered national health insurance reimbursement on May 20, 2026 at ¥55,306,737 per patient.
For sixty years, Parkinson’s disease (PD) treatment has rested on three pillars: levodopa and other dopamine-targeting drugs, deep brain stimulation, and physical/occupational therapy. None of these regenerates the dopamine neurons that PD progressively destroys.
In 2026, that changed.
On April 16, 2026, Nature published the Kyoto University Phase I/II trial of allogeneic iPS-cell-derived dopaminergic progenitors in seven Parkinson’s patients, with 24 months of follow-up — the clinical foundation for Amchepry’s regulatory approval.[¹]
On May 20, 2026, Japan’s MHLW listed Amchepry on the national health insurance reimbursement schedule at ¥55,306,737 per patient — the first iPS-derived regenerative medicinal product approved and reimbursed by any national health system worldwide.
For Parkinson’s patients, cell-replacement therapy has moved from “promising future technology” to “a treatment approved and reimbursed somewhere on Earth.” Whether that “somewhere” is accessible to you is the question this article addresses.
How Amchepry works — iPS-derived dopaminergic cells delivered by stereotactic brain surgery
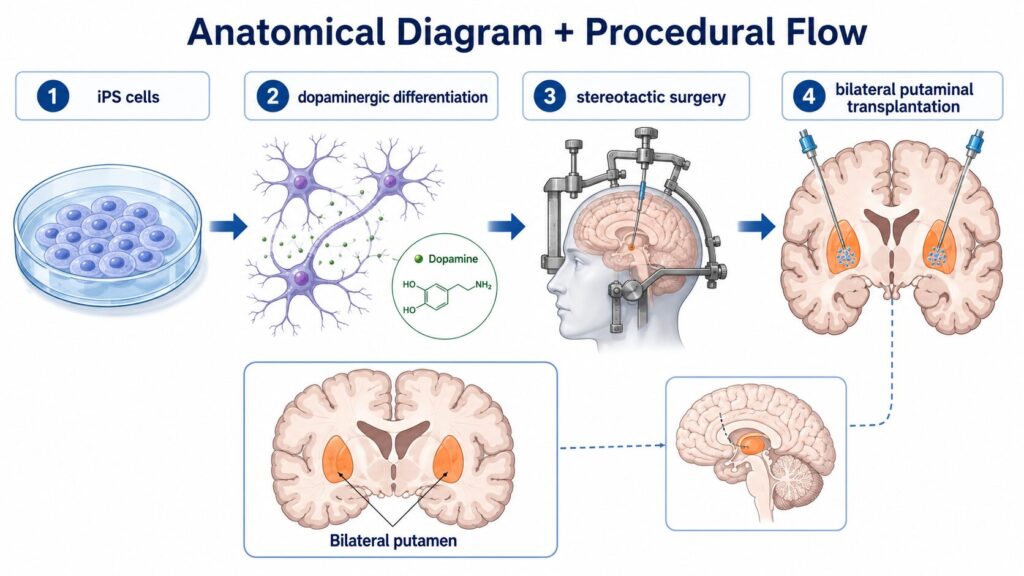
Direct AnswerAmchepry is made by differentiating allogeneic induced pluripotent stem (iPS) cells into dopaminergic neural progenitors, which are then transplanted bilaterally into the putamen through stereotactic brain surgery under general anaesthesia. It is a cell-replacement approach: rather than supporting surviving neurons, it adds new dopamine-producing cells.
Cell source
Amchepry’s active ingredient is dopaminergic neural progenitor cells differentiated from a clinical-grade allogeneic iPS cell line developed by Kyoto University’s Center for iPS Cell Research and Application (CiRA). Importantly, the donor iPS cells used in the Kyoto Phase I/II trial carried homozygous HLA haplotypes — a strategy designed to reduce immune rejection across more recipients.
Delivery: stereotactic brain surgery
The cells are not delivered by infusion or injection. The procedure is a stereotactic neurosurgical operation under general anaesthesia:
- A small burr hole is made in the skull
- Under stereotactic guidance, a fine needle is advanced into the putamen (a deep brain structure)
- Progenitor cells are deposited at multiple sites in both putamina (bilateral transplantation)
Phase I/II results (Sawamoto et al., Nature 2025)
- Patients: 7 (ages 50–69) with idiopathic Parkinson’s disease responsive to levodopa
- Follow-up: 24 months
- Serious adverse events: None
- Mild–to–moderate adverse events: 73 total
- Efficacy (among 6 patients evaluable for efficacy):
- MDS-UPDRS Part III improved in the OFF state in 4 of 6 patients
- MDS-UPDRS Part III improved in the ON state in 5 of 6 patients
- Mean OFF-state improvement: 9.5 points (20.4%)
- Mean ON-state improvement: 4.3 points (35.7%)
- Hoehn-Yahr stage improved in 4 of 7 patients
- Imaging: F-DOPA influx rate constant (K) increased by 44.7% in the putamen, with greater increases in the high-dose group — direct evidence that grafted cells survived and produced dopamine
- No graft overgrowth on MRI
Can international patients get Amchepry in Japan? The honest answer
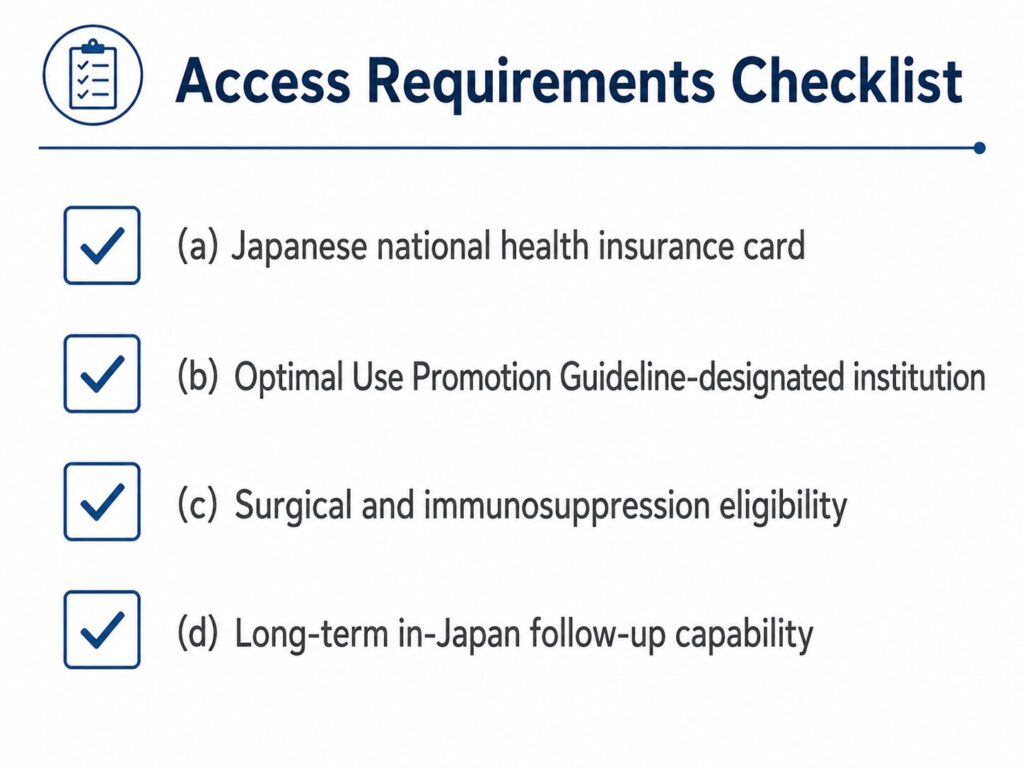
Direct AnswerPractically, no — at least not in 2026. Amchepry’s ¥55.3 million price is currently structured around Japan’s national health insurance coverage; international self-pay access has not been established, and the procedure requires a stereotactic-surgery-capable institution under Japan’s “Optimal Use Promotion Guideline.” Foreign patients should regard Amchepry as a Japan-domestic option in 2026, not a medical-tourism destination.
This is the section international readers come for, so let’s be direct.
The ¥55.3 million sticker shock — and why it matters less than you’d think (for Japanese residents)
The drug-only cost of Amchepry is ¥55,306,737 per patient (about $350,000 USD at typical 2026 exchange rates). Inpatient stay, the stereotactic surgical procedure, pre- and post-operative imaging, and lifelong follow-up costs are billed separately.
For a Japanese resident with a national health insurance card, Japan’s High-Cost Medical Expense Benefit System (高額療養費制度) caps monthly out-of-pocket spending based on income tier. A typical middle-income patient pays only tens of thousands to a few hundred thousand yen out of pocket per month, with the rest absorbed by the insurance system.
For a non-resident foreign patient, that financial structure does not apply. A self-pay international patient would, in principle, face the full ¥55.3 million drug cost plus all surgical and hospitalisation fees — not as an insurance co-pay, but as a complete bill.
The institutional access barrier
Even setting cost aside, Amchepry’s conditional approval comes with “Optimal Use Promotion Guideline” restrictions. Only institutions that meet specific criteria — including functional neurosurgical teams capable of stereotactic transplantation, neurology departments with PD expertise, immunology consultation, and long-term registry follow-up — can administer it.
As of mid-2026, Sumitomo Pharma and MHLW have not published a public English-language pathway for international patients to access Amchepry. There is no equivalent of the “medical tourism” infrastructure that exists for, say, knee osteoarthritis stem cell therapy in Japan.
The 7-year window
Amchepry’s approval is conditional and time-limited — for up to seven years — during which Sumitomo Pharma is required to conduct Phase IV post-marketing studies and submit additional data. Within that window, additional safety and effectiveness data will accumulate, and pricing and access models may evolve.
Realistic 2026 takeaway: The breakthrough is genuinely historic — but the access window for international patients is, in practical terms, closed for now. Watch the next 3–5 years.
Deep brain stimulation (DBS) for Parkinson’s — what it does, what it doesn’t
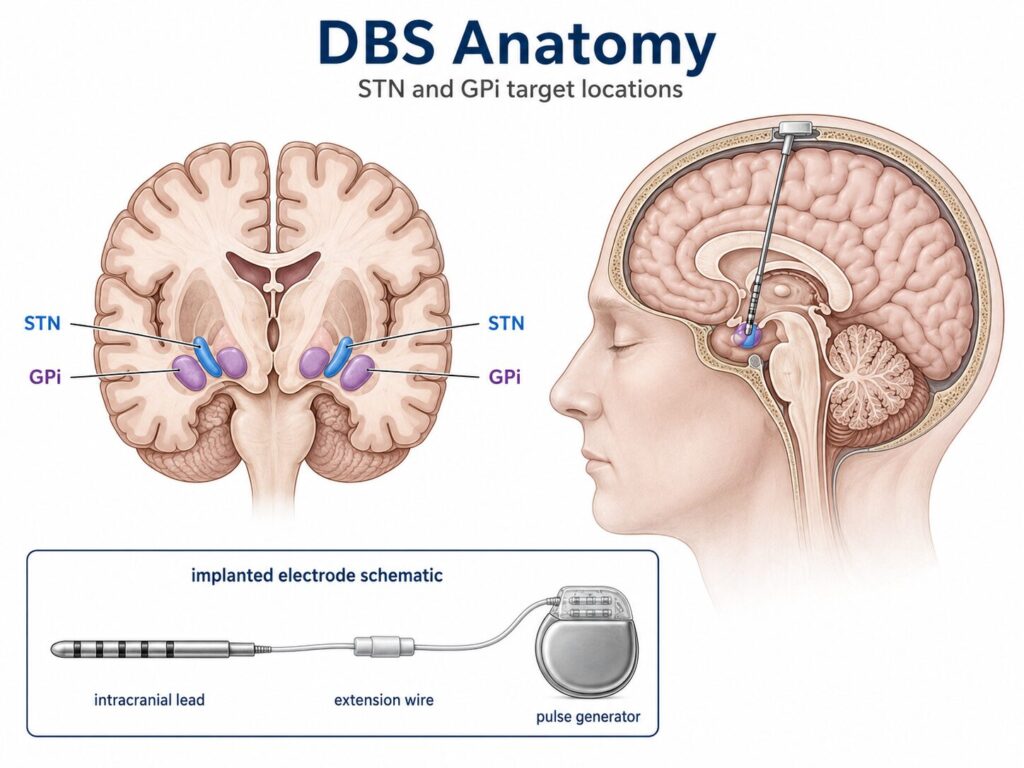
Direct AnswerDeep brain stimulation (DBS) delivers continuous electrical pulses to deep brain nuclei — most commonly the subthalamic nucleus (STN) or globus pallidus internus (GPi) — via surgically implanted electrodes, reliably reducing motor fluctuations and dyskinesias in advanced Parkinson’s disease. DBS does not replace lost dopamine neurons; it modulates the surviving motor network.
DBS has been a clinical standard for advanced Parkinson’s disease since the late 1990s. For internationally mobile patients comparing options, three points matter.
What DBS does well
- Reduces “off” time and motor fluctuations
- Reduces levodopa-induced dyskinesias (often via the medication reduction permitted by improved control)
- Reduces tremor and rigidity, particularly with STN stimulation
- Approved and available in dozens of countries, including the US, UK, EU, Japan, Australia, and most APAC markets
What DBS does not do
- Does not regenerate dopamine neurons
- Does not slow the underlying neurodegeneration
- Limited effect on axial symptoms such as gait freezing, postural instability, speech, and cognitive symptoms
- Carries surgical risks (haemorrhage, infection, device-related complications) and lifelong follow-up requirements
Where DBS sits relative to Amchepry
Both DBS and Amchepry involve stereotactic neurosurgery and general anaesthesia. They differ fundamentally in what is implanted: DBS implants a device (an electrode); Amchepry implants cells. For a patient who declines open-skull surgery, neither approach is the answer.
Mesenchymal stem cell (MSC/ADSC) therapy for Parkinson’s — mechanism, evidence, what’s realistic
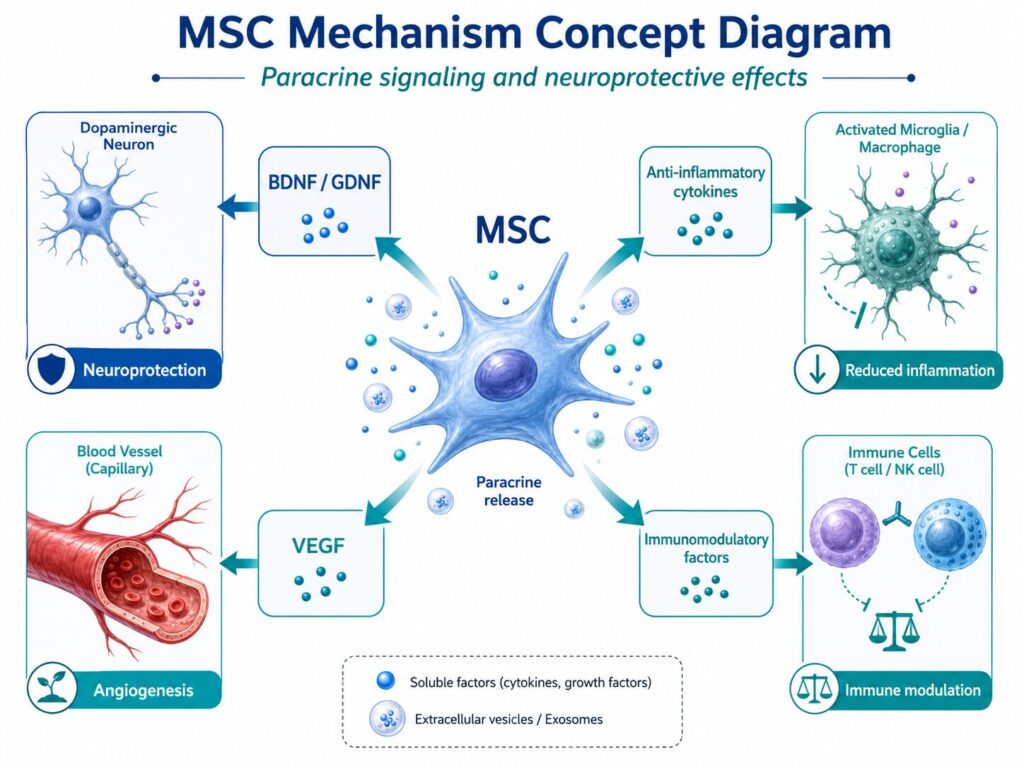
Direct AnswerUnlike Amchepry, which aims to replace lost dopamine neurons, mesenchymal stem cells (MSCs) — including adipose-derived stem cells (ADSCs) — primarily aim to protect surviving neurons through neurotrophic factor release, anti-inflammatory cytokine secretion, and immune modulation. They are typically delivered through intravenous infusion, not brain surgery.
Proposed mechanism
MSCs are not believed to differentiate into dopamine neurons in significant numbers in vivo. Their proposed therapeutic action is paracrine — that is, they release a cocktail of bioactive molecules that:
- Provide neurotrophic support (BDNF, GDNF, and other factors that help surviving neurons stay alive)
- Reduce chronic neuroinflammation through anti-inflammatory cytokines and modulation of microglial activation
- Promote vascular health and support cerebral perfusion through angiogenic signals (e.g., VEGF)
- Provide immunomodulation that may attenuate the chronic immune dysregulation observed in PD
This is a fundamentally different therapeutic concept from cell-replacement: rather than adding new dopamine producers, MSC therapy aims to slow loss of those that remain.
What the clinical evidence shows — and what it does not
Schiess et al. (Movement Disorders 2021) reported a 52-week Phase 1 trial of allogeneic bone marrow-derived mesenchymal stem cells (BM-MSCs) delivered by single intravenous infusion in 20 patients with mild-to-moderate idiopathic Parkinson’s disease. Doses escalated from 1 × 10⁶ to 10 × 10⁶ cells/kg.
- No serious infusion reactions or donor-specific HLA antibodies
- Most common treatment-emergent adverse events: dyskinesias (20%) and hypertension (20%)
- One serious adverse event (asymptomatic chronic lymphocytic leukaemia in a patient with a 4-year pre-existing lymphocytosis history) was deemed possibly related
- At the highest dose, OFF-state UPDRS motor scores improved by 14.4 points (P < 0.01) and total UPDRS by 20.8 points (P < 0.05) at 52 weeks
- Peripheral inflammation markers (TNF-α, CCL22) decreased; BDNF increased
Important note: Schiess et al. used bone marrow-derived MSCs, not adipose-derived MSCs. The two cell sources share core MSC characteristics but differ in expression profiles, ease of harvest, and clinical operational considerations. Findings from BM-MSC trials should not be directly transferred to ADSC.
Vij et al. (Cytotherapy 2025) reported a Hope Biosciences expanded-access program of autologous adipose-derived MSC (HB-adMSC) therapy in elderly Parkinson’s patients. The sample size was small — only 10 patients aged 76–95, who each received six intravenous infusions of 200 million autologous HB-adMSCs over 18 weeks, with end-of-study at week 26.
- Safety: 37 of 46 adverse events were mild; 5 SAEs were reported, none attributed to the drug; no deaths
- Important limitation: The trial was not powered to demonstrate statistical efficacy. Clinically meaningful effect-size signals (effect size > 0.3) were observed on MDS-UPDRS Part I and III, PDQ-39, and PHQ-9, but did not reach statistical significance.
- The authors concluded that a larger randomized placebo-controlled study is needed before efficacy claims can be made.
This is the most directly relevant ADSC trial in the PD literature, but the n = 10 sample size and lack of statistical power must be emphasised in any honest reading.
Wang et al. (Journal of Translational Medicine 2023) performed a systematic review and meta-analysis of cell-therapy trials for Parkinson’s disease, including 11 trials with 210 patients. The analysis found beneficial effects on disease severity and motor function in the OFF state at 3-, 6-, 12-, and 24-month follow-ups, with motor improvement persisting at 36 months. Between 61.6% and 100% of patients across these trials were levodopa responders.
Zhao et al. (Frontiers in Neurology 2024) included 9 controlled trials with 129 patients and reported a weighted mean difference of −14.86 (95% CI: −16.62 to −13.10; P < 0.00001) in motor scores, with effectiveness sustained for at least 12 months. Effective cell sources included neural stem cells, umbilical cord MSCs, and bone marrow MSCs.
The honest summary
MSC/ADSC therapy for Parkinson’s disease is supported by promising mechanistic rationale, encouraging safety data, and meta-analytic signals of motor improvement at 12–24 months. It is not yet supported by adequately powered randomized placebo-controlled trials demonstrating definitive efficacy. Patients considering MSC/ADSC therapy should be informed of both the rationale and the evidence limits.
Stem Cell Therapy in Japan: Plans, Pricing & What to Expect Read GuideSide-by-side: Amchepry vs DBS vs MSC/ADSC
Direct AnswerAmchepry targets dopamine neuron loss directly but requires open-skull surgery, immunosuppression, and Japanese insurance access. DBS modulates motor circuits via implanted electrodes — also surgical, but with decades of clinical track record and worldwide availability. MSC/ADSC therapy aims to protect surviving neurons through non-surgical IV infusion. Each fits a different patient profile, disease stage, and risk tolerance.
| Attribute | AmchepryiPS · Sumitomo · Japan | DBSDeep Brain Stimulation | ADSC / MSCAdipose MSC · IV Infusion |
|---|---|---|---|
| Cell or deviceSource | Allogeneic iPS-derived dopaminergic progenitors | Implanted electrode (no cells) | Autologous adipose-derived MSCs (your own) |
| DeliveryRoute | Bilateral putamen, stereotactic surgery | DBS lead in STN or GPi, stereotactic surgery | Outpatient IV infusion (or intrathecal) |
| Invasiveness | High — open skull, GA | High — skull, GA, lifelong device | Low — outpatient IV |
| Immunosuppression | Yes (tacrolimus monotherapy)2 | No | No (autologous) |
| Regulatory status | MHLW conditional, time-limited (May 2026) | Established standard of care, multiple countries | MHLW Type 2 notification basis (Japan) |
| Primary evidence | Sawamoto Nature 2025, n=7, 24 mo, 4–5 of 6 improved1 | Decades of RCTs and meta-analyses | Schiess (n=20, BM-MSC)3; Vij (n=10, small)4; Wang MA (n=210)5; Zhao MA (n=129)6 |
| International access2026 reality | (self-pay, MHLW Type 2) |
||
| CostIndicative | ¥55.3M (~$350K USD) + surgery + hospitalisation |
Insurance + device cost Varies by country |
Self-pay Varies by clinic and protocol |
All cited evidence verified through PubMed in May 2026. Full references with DOI links are provided at the end of this article.
How to read this table
- If you are eligible for, and willing to accept, brain surgery and immunosuppression, and live in Japan or can establish long-term Japan-based follow-up, Amchepry deserves a formal eligibility evaluation through your Japanese neurologist.
- If you have moderate-to-advanced PD with motor fluctuations, and DBS has been recommended by your movement-disorder neurologist, DBS remains a well-established, country-flexible standard.
- If you want a non-surgical adjunctive approach to support overall systemic state, neuroinflammation, and cerebral perfusion alongside your standard PD care, MSC/ADSC therapy may merit consideration — with full understanding of its current evidence limits.
What the clinical evidence actually says — trials, meta-analyses, and the honest limits
Direct AnswerThe 2025 Nature trial by Sawamoto et al.1 demonstrated safety and signals of efficacy in 7 patients followed for 24 months — promising, but small. Two 2023–2024 meta-analyses of older cell-therapy trials (Wang5, 210 patients; Zhao6, 129 patients) suggest cell therapy improves motor scores at 12–24 months. None of these prove a cure, and adequately powered randomised Phase 3 trials are still pending.
Cell-replacement (iPS) — Phase I/II level
The Sawamoto Phase I/II trial is technically and ethically remarkable: it demonstrates that allogeneic iPS-derived dopaminergic progenitors can be transplanted into the human brain, survive, produce dopamine, and not form tumours over 24 months. It is not a confirmatory efficacy trial. The number of patients is small (n=7), the study is open-label, and definitive Phase 3 efficacy testing is still ahead — to be accumulated through Amchepry’s conditional 7-year approval window and Phase IV post-marketing studies.
MSC-based therapy — Phase 1 and meta-analytic level
The Schiess Phase 1 BM-MSC trial established safety of a single IV infusion in 20 PD patients across four dose tiers, with motor improvements at the highest dose. The Vij expanded-access ADSC study — with only 10 elderly patients and explicitly underpowered for efficacy — established safety but did not reach statistical significance on motor or quality-of-life endpoints. The Wang (n=210) and Zhao (n=129) meta-analyses of older cell-therapy trials point to durable motor benefits at 12–24 months.
What does not exist yet
A large, randomised, placebo-controlled Phase 3 trial of MSC/ADSC therapy in idiopathic Parkinson’s disease, powered to demonstrate definitive efficacy, has not yet been completed and published. Until it is, MSC/ADSC for PD remains an option with promising signals — not a proven cure.
What this means for patient decisions
- Be cautious of any clinic promising “cure” or “reversal” of Parkinson’s disease. No therapy in this article — Amchepry, DBS, or MSC/ADSC — has been shown to cure or reverse PD.
- Be cautious of efficacy claims that go beyond what the evidence supports. A safety-and-feasibility Phase I trial is not the same as a confirmatory Phase 3 trial.
- Be cautious of clinics that present small case series (n < 30) as if they were definitive evidence.
Honest expectation-setting is the most protective thing a clinician can offer.
What Cell Grand Clinic can — and cannot — offer Parkinson’s patients
Direct AnswerCell Grand Clinic does not currently offer Amchepry, DBS, or a Parkinson’s-specific MSC treatment program. Parkinson’s is not among our 13 MHLW-notified regenerative medicine protocols. What we can offer Parkinson’s patients is adjunctive supportive care for Parkinson’s-associated frailty and pre-frailty, cerebral perfusion, and overall systemic state, under separately notified MHLW protocols — alongside, not in place of, your standard neurology care.
We believe the most useful thing a regenerative-medicine clinic can do for an internationally based Parkinson’s patient is to be honest about scope. Here is ours.
What we do NOT offer
| Treatment | At Cell Grand Clinic? |
|---|---|
| Amchepry (iPS) for Parkinson’s | ❌ Not offered. We do not perform iPS cell therapy at all. |
| Deep Brain Stimulation (DBS) | ❌ Not offered. We refer to specialist neurosurgical centers when indicated. |
| Parkinson’s-specific MSC/ADSC program | ❌ Not part of our MHLW-notified protocols. We do not offer a treatment program directly targeting Parkinson’s disease itself. |
What we DO offer — as supportive care, not as a Parkinson’s treatment
| Service | MHLW basis | Purpose |
|---|---|---|
|
Autologous ADSC for Parkinson’s-associated frailty and pre-frailty
Up to 200 million autologous adipose-derived stem cells, cultured over 7 weeks · delivered intravenously
|
MHLW Type 2 PB5250049 · Frailty |
Support muscle mass, mitochondrial function, and overall physical reserve in patients who develop frailty or pre-frailty during PD progression. |
|
Autologous ADSC for atherosclerosis / vascular health
Autologous adipose-derived stem cells · intravenous protocol for vascular regeneration
|
MHLW Type 2 PB5250051 · Atherosclerosis |
Support vascular health, which may indirectly support cerebral perfusion. |
|
Exosome IV / intranasal therapy
30-minute infusion · no fat harvest required · lowest-threshold option
|
Adjunctive Outside Regen-Med Act |
Low-threshold neuroinflammation modulation; 30-minute IV; no fat harvest required. |
|
NMN (nicotinamide mononucleotide) IV
NAD+ precursor protocol · whole-body cellular energy support
|
Nutritional Regenerative protocol |
Mitochondrial support via NAD+ precursor. |
|
English consultation with Dr. Wakabayashi
Written case review · 1–3 business days · direct physician response
|
Consultation English · no interpreter |
3,000+ ADSC cases · ABRM-certified · NIH alumnus. Honest assessment of whether Cell Grand Clinic’s supportive-care protocols are appropriate for your case. |
Considering supportive care alongside your standard Parkinson’s treatment?
Written case review from Dr. Wakabayashi — in English, within 1–3 business days.
What we can offer Parkinson’s patients (adjunctive supportive care only):
- Autologous ADSC for Parkinson’s-associated frailty and pre-frailty (MHLW Type 2 PB5250049)
- Autologous ADSC for atherosclerosis / vascular health (PB5250051)
- Exosome IV or intranasal therapy
- NMN IV (NAD+ precursor for mitochondrial support)
How a case review works.
Share your current Parkinson’s stage, medications, and treatment goals. Dr. Wakabayashi reviews each international inquiry and responds with a written feasibility assessment, a recommended adjunctive supportive care plan, and a transparent quote. Typical turnaround: 1–3 business days.
Frequently asked questions
Q1. Is Amchepry approved outside Japan?
No. As of mid-2026, Amchepry (Sumitomo Pharma’s iPS-derived dopaminergic progenitor product) is approved only under Japan’s conditional, time-limited regulatory pathway. No equivalent regulatory approval has been issued by the US FDA, EMA, UK MHRA, or other national authorities.
Q2. Can a US, UK, or EU patient travel to Japan to get Amchepry?
Not in 2026, in any practical sense. Amchepry is reimbursed under Japan’s national health insurance system, which requires Japanese insurance enrolment. There is no published international self-pay pathway. The institutional access is restricted to designated facilities under MHLW’s Optimal Use Promotion Guideline.
Q3. How much does Amchepry cost?
The drug-only price set by the Japanese Central Social Insurance Medical Council is ¥55,306,737 per patient. Surgical, hospitalisation, and follow-up costs are billed separately. For Japanese residents, out-of-pocket spending is reduced substantially by the High-Cost Medical Expense Benefit System. For self-pay foreign patients, no equivalent system applies.
Q4. What does Amchepry’s “conditional, time-limited approval” mean?
Japan’s conditional and time-limited approval pathway allows regenerative medicinal products with established safety and a reasonable expectation of efficacy to be approved early — for up to seven years — during which the manufacturer must conduct post-marketing studies and submit additional data. After the conditional window, regulators decide whether to grant standard approval based on the accumulated evidence.
Q5. Is stem cell therapy for Parkinson’s safe?
Across the Amchepry Phase I/II trial (Sawamoto et al.[¹]) and the MSC trials (Schiess[³], Vij[⁴]) reviewed in this article, no treatment-related serious adverse events were reported in the cell-replacement cohort, and adverse events in the MSC trials were predominantly mild. Stereotactic surgery itself carries the standard risks of any open-skull neurosurgical procedure (haemorrhage, infection, anaesthesia). Intravenous MSC infusion carries low procedural risk, though the long-term safety of repeated infusions remains an area of ongoing study.
Q6. Does mesenchymal stem cell (MSC/ADSC) therapy cure Parkinson’s?
No. No therapy currently available — Amchepry, DBS, or MSC/ADSC — has been shown to cure or reverse Parkinson’s disease. MSC/ADSC therapy aims to support neuroprotection and overall systemic state. Clinical efficacy in adequately powered randomized placebo-controlled trials has not yet been demonstrated. Patients considering MSC/ADSC therapy should be informed of both the mechanistic rationale and the evidence limits.
Q7. Does Cell Grand Clinic offer Parkinson’s stem cell therapy?
No, not for Parkinson’s disease itself. Parkinson’s is not among our 13 MHLW-notified regenerative medicine protocols. We do offer autologous ADSC under our frailty protocol (PB5250049) for Parkinson’s-associated frailty and pre-frailty, our atherosclerosis protocol (PB5250051), exosome therapy, and NMN IV — as adjunctive supportive care alongside, not in place of, your standard neurology care. We are happy to provide a second opinion and refer to Amchepry- or DBS-capable specialist centers when appropriate.
Summary — hope, honesty, and what comes next
The science is moving. In ten years, the picture for Parkinson’s patients will likely look meaningfully different from today. In 2026, however, three things remain true:
- The breakthrough is real but not portable. Amchepry’s approval in Japan is historic, but it is structured around Japan’s insurance system and does not, in 2026, offer a realistic medical-tourism pathway for non-Japanese patients.
- Phase 3 efficacy data are still pending. Amchepry’s approval is conditional and time-limited, and definitive confirmatory data are expected over the next several years.
- Supportive care is not nothing. Maintaining physical reserve, vascular health, and overall systemic state is a legitimate and clinically meaningful goal during the years before — and likely after — definitive cell-replacement therapy becomes broadly accessible.
Patients are best served by clinicians who are honest about both the science and the access reality.
References
- Sawamoto N, Doi D, Nakanishi E, et al. Phase I/II trial of iPS-cell-derived dopaminergic cells for Parkinson’s disease. Nature. 2025;641(8064):971–977. DOI: 10.1038/s41586-025-08700-0. PMID: 40240591.
- Morizane A, Yamasaki E, Shindo T, et al. Control of immune response in an iPSC-based allogeneic cell therapy clinical trial for Parkinson’s disease. Cell Stem Cell. 2025;32(9):1346–1355.e3. DOI: 10.1016/j.stem.2025.07.012. PMID: 40834856.
- Schiess M, Suescun J, Doursout MF, et al. Allogeneic Bone Marrow–Derived Mesenchymal Stem Cell Safety in Idiopathic Parkinson’s Disease. Movement Disorders. 2021;36(8):1825–1834. DOI: 10.1002/mds.28582. PMID: 33772873.
- Vij R, Kim H, Park H, et al. Safety and efficacy of adipose-derived mesenchymal stem cell therapy in elderly Parkinson’s disease patients: an intermediate-size expanded access program. Cytotherapy. 2025;27(2):181–187. DOI: 10.1016/j.jcyt.2024.09.004. PMID: 39425736.
- Wang F, Sun Z, Peng D, et al. Cell-therapy for Parkinson’s disease: a systematic review and meta-analysis. Journal of Translational Medicine. 2023;21(1):601. DOI: 10.1186/s12967-023-04484-x. PMID: 37679754.
- Zhao J, Qu K, Jia S, et al. Efficacy and efficacy-influencing factors of stem cell transplantation on patients with Parkinson’s disease: a systematic review and meta-analysis. Frontiers in Neurology. 2024;15:1329343. DOI: 10.3389/fneur.2024.1329343. PMID: 38682036.
Updated: 2026.06.06