Inquiries by Email
Inquiries by Email
Stem cell therapy for diabetic and peripheral neuropathy uses adipose-derived mesenchymal stem cells to reduce neuroinflammation, promote axonal regrowth, and restore nerve conduction velocity in patients whose drugs have stopped working.
Below: whether nerve damage can truly be reversed, how regenerative stem cell therapy repairs nerves instead of masking pain, what results patients can realistically expect, and what treatment in Japan involves.
Cell Grand Clinic in Osaka, Japan cultures up to 200 million autologous stem cells from your own minimal fat tissue over 7 weeks, delivered via IV — never donor cells.
- Can Neuropathy Be Reversed?
- What Is Stem Cell Therapy for Diabetic & Peripheral Neuropathy?
- Why Conventional Drugs Don’t Stop Nerve Damage
- Types of Neuropathy That May Respond to Stem Cell Therapy
- How Stem Cells Target Nerve Pain at Its Source
- What Are the Latest Treatments for Peripheral Neuropathy?
- Does Stem Cell Therapy Work for Diabetic Neuropathy? What Clinical Trials Show
- Who May Benefit — and What to Expect
- Why Japan — and Why Cell Grand Clinic?
- The Treatment Protocol for International Patients
- Frequently Asked Questions
- Take the Next Step
- References
Can Neuropathy Be Reversed?
Some neuropathy can be partially reversed — especially early peripheral and diabetic neuropathy, where the nerves are damaged but not yet lost. Standard drugs (gabapentin, pregabalin, duloxetine) only mask the pain; they do not repair nerves. Regenerative stem cell therapy using adipose-derived mesenchymal stem cells (ADSCs) works differently: it reduces nerve inflammation, restores blood supply, and supports axon regrowth — which can improve sensation and ease pain. Advanced, long-standing nerve loss is much harder to reverse, and results vary by individual.
What Is Stem Cell Therapy for Diabetic & Peripheral Neuropathy?
Stem cell therapy for diabetic and peripheral neuropathy is an innovative regenerative approach that uses mesenchymal stem cells (MSCs) — most commonly adipose-derived (ADSCs) — to reduce nerve inflammation, support axonal regrowth, and improve nerve conduction velocity in patients whose pain medications no longer provide relief.

But here is what most patients do not realize: these cells do not replace damaged neurons one-for-one. The real story is that your own cells can release the signals that medication never delivers — growth factors, anti-inflammatory cytokines, and exosomes that quiet the chronic neuroinflammation behind nerve pain. Let us start with why conventional drugs hit a ceiling.
Why Conventional Drugs Don’t Stop Nerve Damage
Your hands tingle at night. Your feet feel numb, as if wrapped in invisible gauze. Medications take the edge off — but never truly restore what was lost. If peripheral neuropathy has stolen your sensation, your balance, or your sleep, you are not alone, and conventional medicine may have already reached its limits for you.

A 2026 review published in JAMA reports that peripheral neuropathy affects approximately 1% of adults worldwide, with prevalence rising sharply among older adults and those with chronic conditions. Diabetes is the single most common cause: diabetic neuropathy is estimated to affect approximately 206 million people worldwide, with diabetes as the leading cause. Over 50% of peripheral neuropathy cases in Western populations are diabetic in origin, and another 27% remain idiopathic — meaning no identifiable cause is ever found, even after a full diagnostic work-up.
Despite these staggering numbers, treatment options remain frustratingly limited. The same JAMA review notes that gabapentin, one of the most widely prescribed medications for neuropathic pain, achieves a 50% or greater reduction in pain intensity in only 38% of patients with painful diabetic peripheral neuropathy at 1,200 mg/day. Many patients cycle through pregabalin, duloxetine, and tricyclic antidepressants — searching for relief that may never fully arrive.
Types of Neuropathy That May Respond to Stem Cell Therapy
Not all neuropathy is the same. The potential for stem cell therapy varies by type, stage, and underlying cause. Based on the current body of research, several forms stand out as particularly relevant.
Diabetic Peripheral Neuropathy (DPN)
Diabetic peripheral neuropathy is the most extensively studied form in the context of stem cell therapy. It typically begins in the feet and progresses upward, causing burning pain, numbness, and loss of protective sensation that can lead to ulcers and amputation. According to the 2026 JAMA review, DPN develops in a substantial proportion of diabetic patients and is the leading cause of non-traumatic lower limb amputation worldwide. Current pharmacological treatments manage symptoms but do not reverse the underlying nerve fiber loss.
Chemotherapy-Induced Peripheral Neuropathy (CIPN)
Cancer survivors frequently develop peripheral neuropathy as a side effect of platinum-based, taxane, or vinca alkaloid chemotherapy agents. CIPN can persist for months or years after treatment ends, affecting up to 68% of patients in the first month and remaining chronic in approximately 30%. No FDA-approved treatment currently exists specifically for CIPN, making it a condition of significant unmet need.
Small Fiber Neuropathy and Idiopathic Neuropathy
Small fiber neuropathy selectively damages the thin, unmyelinated nerve fibers responsible for pain and temperature sensation. It causes burning pain, often in a “stocking-and-glove” distribution, and is notoriously difficult to diagnose with standard nerve conduction studies. For the 27% of neuropathy patients whose condition is classified as idiopathic — no known cause — treatment options are especially limited, as there is no underlying disease to target.
How Stem Cells Target Nerve Pain at Its Source
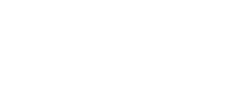
A 2025 review published in Frontiers in Cell and Developmental Biology provides a comprehensive overview of how mesenchymal stem cells (MSCs) interact with damaged peripheral nerves. The mechanisms are multifaceted.
Neurotrophic factor secretion. MSCs release brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF) — two proteins that are critical for the survival, growth, and repair of neurons. These factors provide a neuroprotective environment around damaged nerve fibers, supporting regeneration rather than further degeneration.
Immunomodulation. Chronic neuropathy is often accompanied by persistent neuroinflammation. MSCs can shift the immune environment from a pro-inflammatory state to a reparative one — specifically by inhibiting M1-type macrophages (which drive inflammation) and promoting M2-type macrophages (which support tissue repair). The review identifies suppression of NF-κB and PI3K/AKT signaling pathways as key mechanisms behind this shift.
Exosomes and secretome. Beyond direct cell-to-cell contact, MSCs release tiny vesicles called exosomes that carry bioactive molecules — cytokines, growth factors, and microRNAs — to distant tissues. These acellular components have demonstrated anti-inflammatory, neuroprotective, and immunomodulatory properties in their own right, suggesting that even the “byproducts” of stem cells may contribute to nerve healing.
Myelin and vascular support. Peripheral nerves depend on intact myelin sheaths for signal conduction and on healthy blood supply for oxygen and nutrients. MSCs have been shown to promote both remyelination and angiogenesis (new blood vessel formation), addressing two fundamental requirements for nerve recovery.
What Are the Latest Treatments for Peripheral Neuropathy?
Beyond gabapentin and pregabalin, the most actively researched 2026 options for peripheral neuropathy include mesenchymal stem cell therapy, exosome-based regenerative medicine, photobiomodulation, and dorsal root ganglion stimulation. A 2024 meta-analysis published in Stem Cell Research & Therapy (7 controlled trials, 5,431 records screened) reported that stem cell therapy improved motor nerve conduction velocity by a weighted mean difference of 2.2 m/s in patients with diabetic peripheral neuropathy.
In plain language: among the new options being studied, stem cell therapy is the only one with a recent meta-analysis showing objective electrical evidence of nerve repair, not just pain reduction. That is why this article focuses on the regenerative pathway.
Does Stem Cell Therapy Work for Diabetic Neuropathy? What Clinical Trials Show
Yes — stem cell therapy has shown measurable improvement for diabetic peripheral neuropathy in human studies. A 2024 randomized controlled trial published in Stem Cell Research & Therapy followed 97 patients with type 2 diabetes for 8 years (NCT01719640) and reported DPN incidence of 10.3% in the stem cell group versus 48.3% in controls (p=0.0015) — meaning treated patients were nearly five times less likely to develop neuropathy.
| Study | Year | Design | Patients (n) | Key Finding | Cell Type |
|---|---|---|---|---|---|
| Alizadeh et al. Stem Cell Res Ther |
2024 | SR & Meta-analysis | 7 trials | Motor NCV +2.2 m/s, Sensory NCV +1.9 m/s, TCSS −3.6 points | BM-MNC, UC-MSC |
| Wu et al. Stem Cell Res Ther |
2024 | RCT, 8-year follow-up | 97 | DPN: 10.3% (MSC) vs 48.3% (control), p=0.0015 | BM-MSC + BM-MNC |
| Li et al. Stem Cell Res Ther |
2025 | Meta-analysis | 34 RCTs | Autologous MSC > allogeneic, OR 4.64 (95% CI 3.42–6.31) | Mixed (DM) |
| Claessens et al. Bioengineering |
2024 | Systematic Review | 10 studies | 7/10 studies showed neuropathic pain reduction (QOL not consistently improved) | Fat graft, SVF (adipose-derived) |
All studies used human subjects. Full references with DOI links are provided at the end of this article.
Nerve Conduction Velocity: Objective Evidence of Repair
The Alizadeh 2024 meta-analysis pooled data from seven controlled clinical trials in human DPN patients. The cell types used were bone marrow-derived mononuclear cells (BM-MNCs) and umbilical cord-derived mesenchymal stem cells (UC-MSCs), administered primarily through intramuscular injection.
- Motor nerve conduction velocity improved by WMD 2.2 m/s (95% CI 1.6–2.8) — meaning electrical signals through motor nerves traveled measurably faster after treatment.
- Sensory nerve conduction velocity improved by WMD 1.9 m/s (95% CI 1.1–2.6) — meaning the nerves responsible for touch and temperature sensation were also recovering.
- Toronto Clinical Scoring System (TCSS) decreased by WMD −3.6 points (95% CI −5.0 to −2.2) — a meaningful drop in symptom burden patients can feel.
- Vibration perception threshold improved by WMD −2.9 (95% CI −4.0 to −1.8).
Reported complications were limited to injection-site pain and mild swelling that resolved within days; no serious adverse events were attributed to the stem cell treatment itself.
8-Year RCT: Long-Term Prevention (Wu 2024)
The Wu et al. trial randomized 97 T2D patients into three groups: bone-marrow MSCs combined with mononuclear cells (n=33), mononuclear cells alone (n=32), or standard medical treatment (n=31). At 8 years, only 10.3% of the combination group developed DPN, versus 17.9% in the MC-only group (p=0.015) and 48.3% in the control group.
Reported adverse events included perioperative abdominal pain, puncture-site bleeding (4 patients, resolved with local pressure), transient fever and chills, and two cases of transient neutropenia within the first year in the combination group. No treatment-related serious adverse events or long-term safety signals (including malignancy or death) emerged over the 8-year follow-up.
It is worth noting that this trial used bone-marrow-derived cells delivered through a more invasive route than the IV protocol used at most clinics today (the cells were infused via interventional catheterization of the dorsal pancreatic artery, plus an IV booster at one week). The cell type and the delivery method both differ from a standard ADSC IV protocol — but the underlying paracrine and regenerative mechanisms are shared across MSC tissue sources.
Stem Cell Therapy for Diabetes: A Regenerative Approach to Glycemic Control Learn MoreWho May Benefit — and What to Expect
Patients with diabetic, idiopathic, chemotherapy-induced, or post-herpetic peripheral neuropathy whose drugs are no longer providing relief may be candidates.
Individual suitability is determined during a medical consultation. This checklist is for general reference only.
Results are not immediate. Most patients begin noticing changes gradually over a period of weeks to months, as the regenerative and anti-inflammatory processes unfold. Some patients choose to undergo a second course of treatment to reinforce the initial response.
Reach us directly — WhatsApp and email inquiries are free of charge.
Why Japan — and Why Cell Grand Clinic?
If you are considering stem cell therapy for neuropathy, the choice of where to receive treatment matters as much as the treatment itself. Stem cell clinics operate in dozens of countries, but regulatory frameworks vary enormously — and the difference can determine both your safety and your results.
Japan stands apart for one critical reason: it is the only major nation with a dedicated legal framework governing regenerative medicine. The Act on the Safety of Regenerative Medicine, enforced by the Ministry of Health, Labour and Welfare (MHLW), requires every clinic offering stem cell treatments to register each therapy plan with the government, undergo review by independent certified committees, and maintain CPC-grade laboratories that meet strict manufacturing standards. This is not voluntary accreditation — it is law.
| Factor | Japan (MHLW Type 2) | Mexico | Thailand |
|---|---|---|---|
| Government Oversight | MHLW Type 2 certified ✓ | Limited regulation | Emerging regulation |
| Cell Quality Standards | CPC-grade, ISCT-verified, 7-week culture ✓ | Varies by clinic | Varies by clinic |
| Cell Count per Treatment | Up to 200 million ✓ | Varies | Varies |
| Autologous (Own Cells) | Yes ✓ | Often allogeneic | Mixed |
| Physician Credentials | NIH-trained MD ✓ | Varies | Varies |
Comparison is based on general regulatory frameworks. Individual clinics may vary. Japan’s MHLW Type 2 certification system (Act on the Safety of Regenerative Medicine) provides government-level oversight applicable to treatments using cultured autologous cells.
Grand Stem Cell: Four Quality Standards
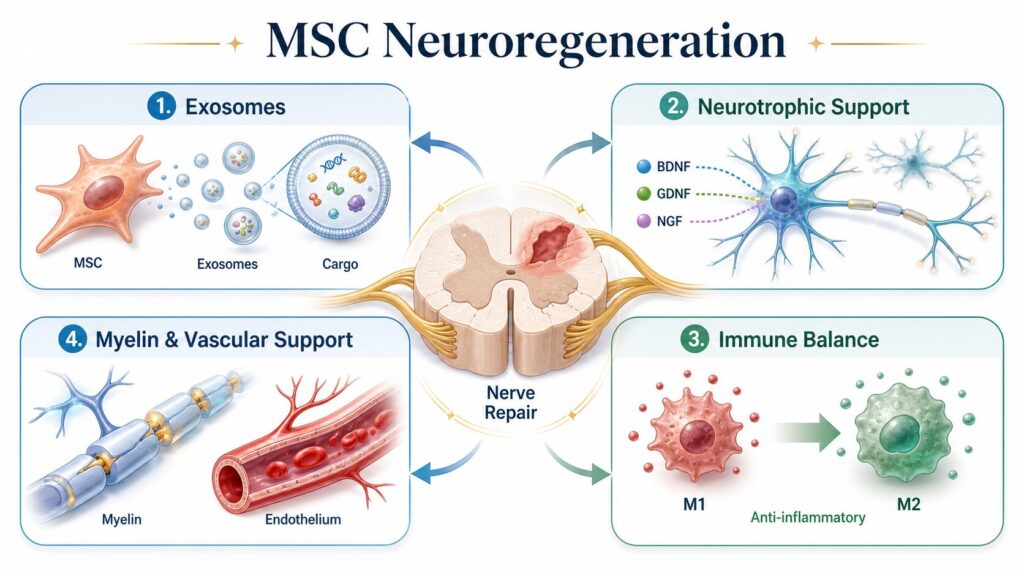
What sets Cell Grand Clinic’s stem cells apart is a commitment to four non-negotiable quality benchmarks that define every Grand Stem Cell treatment:
Cultured Exclusively for You. Grand Stem Cells are never off-the-shelf or shared. After your treatment plan is decided, cells are cultured exclusively from your own adipose tissue over a 7-week period. Every cell is grown for one patient and one patient only.
ISCT-Standard Verification. Surface marker testing follows the International Society for Cellular Therapy (ISCT) global standard, confirming that every administered cell is a genuine mesenchymal stem cell. Cells that do not meet criteria are discarded.
95%+ Viability — Only Living Cells. Dead or degraded cells cannot contribute to tissue repair. Cell Grand Clinic verifies that viability remains above 95% right up to the moment of administration, maintaining quality control through the final step.
Youth and Volume, Without Compromise. Stem cells age with repeated culturing, losing regenerative capacity. Grand Stem Cells are strictly limited to Passage 3 or below, and up to 200 million cells are cultured while preserving their youthful activity and potency.
Every patient receives a Certificate of Quality documenting that their Grand Stem Cells have met all four standards.
Cell Quality: The Key Factor That Impacts Stem Cell Therapy Outcomes Learn MoreCell Grand Clinic operates under MHLW Type 2 certification (CPC License FA5250001) — the higher-tier classification within the Act, applicable to treatments using cultured autologous cells — under the medical direction of M.D., Ph.D. Yuichi Wakabayashi, who completed postdoctoral training at the National Institutes of Health (NIH) in the United States and holds board certification from the American Board of Regenerative Medicine (ABRM).
The Treatment Protocol for International Patients
The treatment process at Cell Grand Clinic involves two visits to Osaka, separated by
approximately seven weeks.
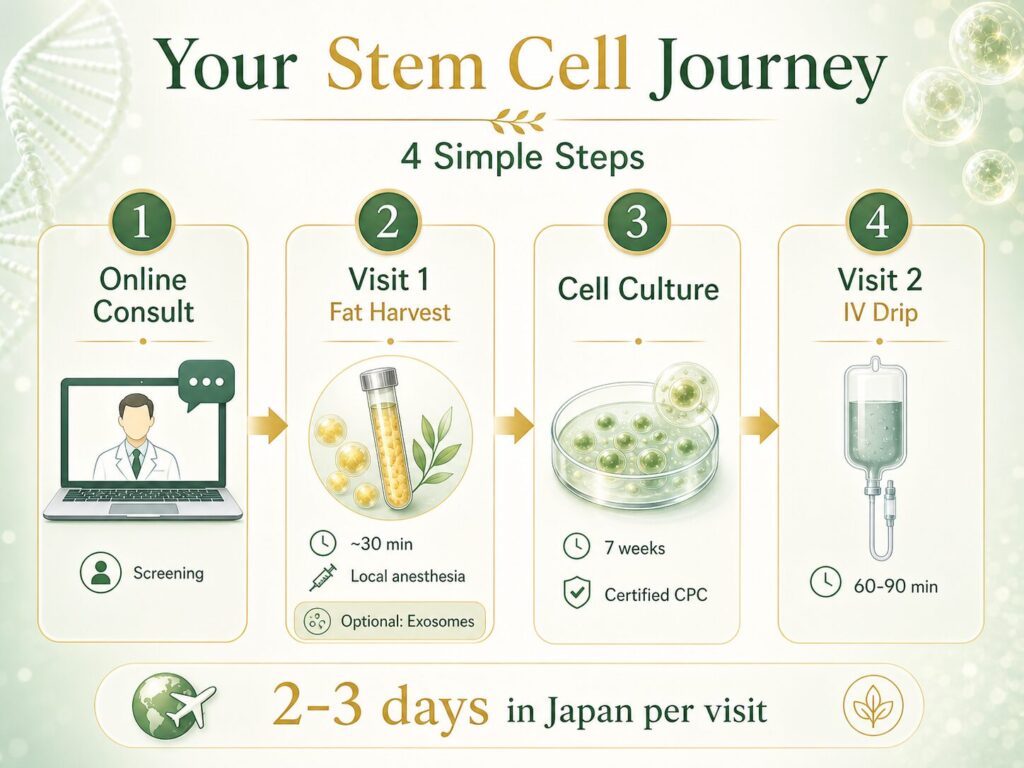
Step 1 — Online Consultation: Remote screening, medical record review, personalized treatment planning.
Step 2 — Visit 1 (Fat Harvest): Tiny size fat harvest (~30 minutes, local anesthesia). Return to your hotel immediately.
On the very same day as your fat collection, you also have the option to receive exosome therapy. Culturing your own stem cells takes several weeks, and many patients don’t want to simply wait while their symptoms continue. Exosomes—the tiny signaling messengers naturally released by stem cells—can help calm inflammation and ease discomfort during this period, so you’re already starting to feel better by the time your cultured cells are ready. Think of it as a bridge: exosomes work with your treatment timeline, not against it.
Step 3 — Cell Culture (7 weeks): Expansion at our certified CPC. Return home during this period.
Step 4 — Visit 2 (Administration): IV drip ± local injection (60–90 minutes).
Total time in Japan: approximately 2–3 days per visit.
Exosome Therapy: Same-Day, Cell-Free Regeneration Learn More Drug-Free ED Treatment: Stem Cells Without Pills or Implants Learn MoreReach us directly — WhatsApp and email inquiries are free of charge.
Frequently Asked Questions
Can stem cells cure neuropathy?
Current evidence suggests that stem cell therapy may help improve nerve function and reduce neuropathic symptoms, but it is not considered a cure. Clinical trials have demonstrated measurable improvements in nerve conduction velocity and symptom scores in patients with diabetic peripheral neuropathy. However, the degree of improvement varies by individual, the type and severity of neuropathy, and how early treatment is initiated. Stem cell therapy is best understood as a regenerative intervention that may slow progression and promote partial nerve repair — not a guaranteed reversal of all damage.
Does stem cell therapy work for diabetic neuropathy?
Clinical research shows promising results. A 2024 meta-analysis of 7 controlled trials found that stem cell therapy significantly improved motor nerve conduction velocity (WMD +2.2 m/s) and sensory nerve conduction velocity (WMD +1.9 m/s) in patients with diabetic peripheral neuropathy. The Toronto Clinical Scoring System, a measure of overall neuropathy severity, also improved significantly. These objective findings suggest that stem cells may help repair nerve damage in diabetic patients, though larger-scale trials are ongoing.
Is stem cell therapy for neuropathy available in Japan?
Yes. Japan is one of the few countries with a government-regulated framework for regenerative medicine. Under the Act on the Safety of Regenerative Medicine, clinics must register treatment plans with the MHLW and meet strict laboratory and safety standards. Cell Grand Clinic in Osaka offers MHLW-certified stem cell therapy using autologous adipose-derived stem cells, and regularly treats international patients traveling from the United States, Europe, the Middle East, and Asia.
What types of stem cells are used for nerve repair?
Research has explored several types, including bone marrow-derived mononuclear cells (BM-MNCs), umbilical cord-derived mesenchymal stem cells (UC-MSCs), and adipose-derived stem cells (ADSCs). Cell Grand Clinic uses adipose-derived stem cells harvested from the patient’s own fat tissue. ADSCs share the same core regenerative mechanisms — neurotrophic factor secretion, immunomodulation, and exosome release — as other mesenchymal stem cell types, while offering the advantage of being autologous (your own cells, reducing rejection risk) and relatively easy to harvest.
How much does stem cell therapy for neuropathy cost in Japan?
Treatment costs vary depending on the specific protocol, the number of cells cultured, and whether additional therapies are combined. Cell Grand Clinic provides a personalized cost estimate after an initial medical review. For details, contact the clinic directly via WhatsApp or email — inquiries are free of charge.
How long until I notice improvement after treatment?
Most patients do not experience immediate results. Because stem cell therapy works through gradual biological processes — reducing inflammation, promoting nerve regeneration, and restoring blood supply — improvements typically emerge over a period of several weeks to three months following treatment. Some patients report continued improvement for up to six months. A second treatment course may be recommended to strengthen and sustain the response.
Can neuropathy be reversed?
It depends on the type and stage. Early peripheral and diabetic neuropathy — where nerve fibers are damaged but still present — has the best chance of partial reversal, because regenerative therapy can repair nerves rather than only blocking pain signals. Long-standing, advanced nerve loss is much harder to reverse. No treatment guarantees a cure, and outcomes vary by individual.
Is neuropathy reversible?
Some neuropathy is reversible to a degree, particularly when treated early and when the underlying cause (such as high blood sugar) is also controlled. Conventional medications manage symptoms but do not reverse nerve damage; regenerative stem cell (ADSC) therapy targets the damage itself by reducing inflammation, improving microcirculation, and supporting nerve regrowth.
Can diabetic neuropathy be reversed?
Early diabetic peripheral neuropathy can sometimes be partially reversed when blood sugar is controlled and nerve repair is supported. Stem cell therapy has improved nerve conduction and symptoms in clinical studies of diabetic neuropathy, though most trials to date use allogeneic MSCs and larger studies are still needed. Advanced diabetic nerve loss is harder to reverse.
Take the Next Step
Living with neuropathy means living with uncertainty — will the numbness spread, will the pain worsen, will your balance continue to decline? If conventional treatments have reached their limit, regenerative medicine may offer a different path forward. Many neuropathy patients also struggle with broader chronic pain — for more on how stem cell therapy addresses pain at its source, see our guide to stem cell therapy for chronic pain.
Cell Grand Clinic’s medical team is available to review your case, discuss whether stem cell therapy may be appropriate for your type of neuropathy, and answer any questions about treatment in Japan.
Reach us directly — WhatsApp and email inquiries are free of charge.
References
- Mauermann ML, Staff NP. Peripheral Neuropathy: A Review. JAMA. 2026;335(3):255-266. https://doi.org/10.1001/jama.2025.19400
- Alizadeh SD, et al. Human studies of the efficacy and safety of stem cells in the treatment of diabetic peripheral neuropathy: a systematic review and meta-analysis. Stem Cell Res Ther. 2024;15(1):442. https://doi.org/10.1186/s13287-024-04033-3
- Wu Z, Huang S, Li S, et al. Bone marrow mesenchymal stem cell and mononuclear cell combination therapy in patients with type 2 diabetes mellitus: a randomized controlled study with 8-year follow-up. Stem Cell Res Ther. 2024;15(1):339. https://doi.org/10.1186/s13287-024-03907-w
- Zhang WJ, Pi XW, Hu DX, Liu XP, Wu MM. Advances and challenges in cell therapy for neuropathic pain based on mesenchymal stem cells. Front Cell Dev Biol. 2025;13:1536566. https://doi.org/10.3389/fcell.2025.1536566
- Claessens AAE, Vriend L, Ovadja ZN, Harmsen MC, van Dongen JA, Coert JH. Therapeutic Efficacy of Adipose Tissue-Derived Components in Neuropathic Pain: A Systematic Review. Bioengineering. 2024;11(10):992. https://doi.org/10.3390/bioengineering11100992
Updated: 2026.06.05