Inquiries by Email
Inquiries by Email
Stem Cells Are Alive. That Changes Everything.
Here is the single most important thing to understand before you choose a stem cell clinic:
Stem cells are not a drug. They are living creatures.
They breathe. They tire. They age. They secrete signals to the tissues around them, and they die if handled badly. You cannot stockpile them on a shelf and assume they will behave the same a year later. And — because they are alive — three things decide whether they actually help you:
- Their quality (are they fresh, alive, and truly stem cells?)
- Their type (where did they come from, and do they match you?)
- Their amount (how many, and is “more” actually “better”?)
The Steak Analogy
The word “steak” on a menu tells you almost nothing. A $10 diner steak and an A5 Wagyu tasting course share a name, but almost nothing else. The gap between them is three things:
- Quality — how the animal was raised, how long the meat was aged, how carefully it was handled before it reached your plate. Most of the price sits here.
- Type — beef, pork, chicken, duck. Each is a completely different animal with a completely different effect on your meal. “Meat” does not describe any of them accurately.
- Amount — 80 grams is a light dinner. 400 grams is an evening you regret. Quantity is not neutral.
Stem cell therapy works on the exact same three axes. “Stem cells” on a clinic’s signboard means almost nothing on its own. What actually decides whether your treatment works — or causes a problem — is quality, type, and amount.
The word “steak” on a menu tells you almost nothing. A $10 diner steak and an A5 Wagyu tasting course share a name, but almost nothing else. The gap between them is three things:
- Quality — how the animal was raised, how long the meat was aged, how carefully it was handled before it reached your plate. Most of the price sits here.
- Type — beef, pork, chicken, duck. Each is a completely different animal with a completely different effect on your meal. “Meat” does not describe any of them accurately.
- Amount — 80 grams is a light dinner. 400 grams is an evening you regret. Quantity is not neutral.
Stem cell therapy works on the exact same three axes. “Stem cells” on a clinic’s signboard means almost nothing on its own. What actually decides whether your treatment works — or causes a problem — is quality, type, and amount.
This article walks through each of those three questions in plain English, then shows how Cell Grand Clinic has built its answers into a single standard called Grand Stem Cell.
Question 1 — What Is the Quality of a Stem Cell?
Stem cell quality means whether the cells are alive when they reach you (viability), whether they are truly mesenchymal stem cells (identity), whether they are free of contaminants (purity), and whether they are still biologically young (passage number). Source tissue matters, but a poorly cultured cell from a “good” source will always lose to a well-cultured cell from a different one.
Before we talk about percentages and scientific acronyms, here is the reality of how stem cells are actually handled between the laboratory and you:
- Two clinics can harvest from the same tissue and release cells with wildly different viability.
- Two clinics can both call their product “stem cells” while only one has actually proven it is still a stem cell.
- Two clinics can sell you “200 million cells” — one hands you 200 million living cells, the other 200 million with a large fraction already dead.
This is the gap the international medical community has been trying to close since 2006, when the International Society for Cellular Therapy (ISCT) published the now-universal minimal criteria for identifying a mesenchymal stem cell — plastic-adherent; positive for CD73, CD90, CD105; negative for CD45, CD34, CD14/11b, CD79α/CD19, HLA-DR; and capable of differentiating into bone, fat, and cartilage lineages. Cells that fail any of these tests are, by definition, not stem cells — regardless of what the label says.
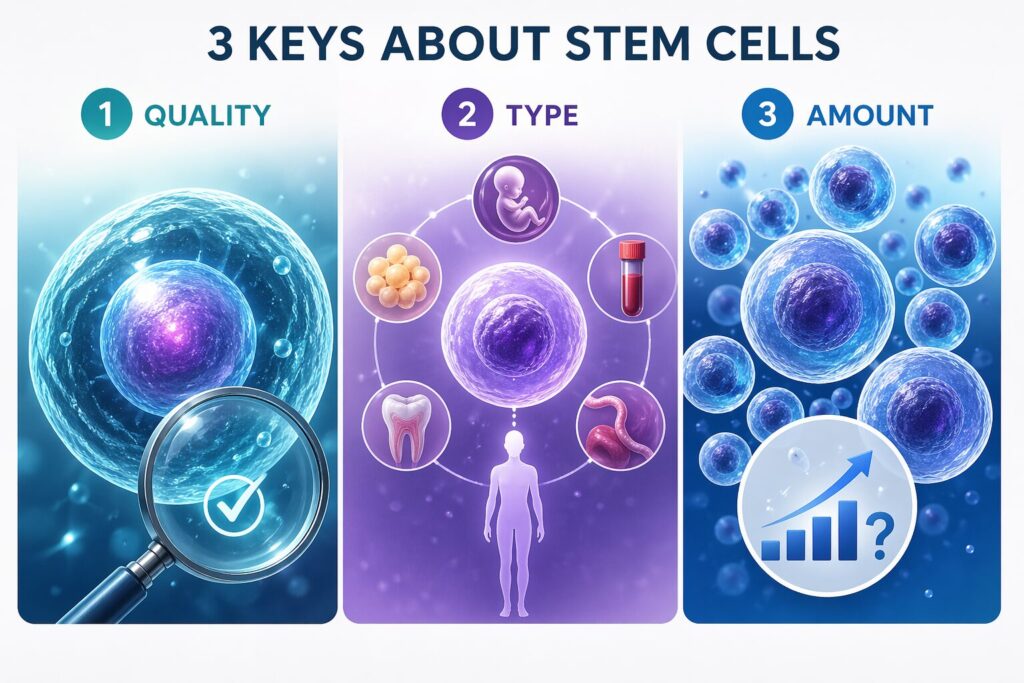
The Grand Stem Cell standard is built on four checkpoints. If you take one thing from this article, take these four.
Pillar 1 — Made Fresh for You. Never Stockpiled.
Some overseas clinics run large batches of donor stem cells in advance, freeze them in small aliquots, and thaw them as customers walk in. This is efficient for the clinic. It is not efficient for your body.
At Cell Grand Clinic, cultivation only starts after your own fat tissue has been harvested. For the next roughly seven weeks, the cells in the incubator exist for one person: you. No pooled donor batches. No six-month-old freezer stock. No shared cultures with other patients.
Living cells are not like tablets. Repeated freeze-thaw cycles bruise them. Long-term storage weakens their secretory function. A batch grown fresh, for you, from you, avoids all of that.
Pillar 2 — Proven Stem Cells, Not Look-Alikes (ISCT Identity Testing)
Here is a quiet truth many clinics do not advertise: a “stem cell” that loses its surface markers during expansion is, biologically, no longer a stem cell. It is a fibroblast-like cell that looks similar under a microscope but behaves very differently in the body. Without identity testing, you cannot tell which you are receiving.
Every Grand Stem Cell batch is checked against the Dominici et al. 2006 criteria published in Cytotherapy (https://doi.org/10.1080/14653240600855905) — the same tests used worldwide in academic research and registered clinical trials:
- Must be present: CD73, CD90, CD105 — typically ≥98% positive in our cultures
- Must be absent: CD45, CD34, CD14/CD11b, CD79α/CD19, HLA-DR — excluding hematopoietic and immune-cell contaminants
We do not just call them stem cells. We prove they are, every single time. Batches that fail are not used — no exceptions, no discounts, no “close enough.”
Pillar 3 — ≥95% Viability (Live Cells Only)
A stem cell can only help you if it is alive when it reaches your tissue. Dead cells do not secrete growth factors, do not home to injury sites, and do not differentiate. Worse, they leave debris that your immune system has to clean up.
Grand Stem Cells are confirmed at ≥95% viability immediately before administration. Viability varies widely across published stem cell products, and “viability at release” is one of the first questions any patient should ask — because the number often tells you more about the laboratory’s discipline than any marketing slogan does.
If you are paying for 200 million cells, you should receive 200 million living cells — not 200 million with a large fraction already dead or dying.
Pillar 4 — Young Cells, Not Over-Passaged (The Point Almost No One Talks About)
This is the pillar almost no marketing page discusses, and it may be the most important of all.
In cell culture, a “passage” is one round of detaching the cells, counting them, and re-seeding them into fresh flasks. Each passage is how the lab grows the population. But each passage is also one step closer to cellular aging.
Research on adipose-derived mesenchymal stromal cells published in Cytotherapy (https://doi.org/10.1016/j.jcyt.2013.07.004) found chromosomal abnormalities (aneuploidy) were essentially absent in freshly isolated cells, but rose to 7.1% at passages 5–16 and reached 19.8% in senescent cultures.
Function follows structure. A separate study in Cytotherapy (https://doi.org/10.1016/j.jcyt.2017.08.007) showed the neuroprotective activity of the MSC secretome is significantly reduced as passage number increases and as donor age rises — two independent drops that compound. Over-expanded cells do not just look older; they lose the very signaling power that is supposed to help you.
The Grand Stem Cell rule:
- Third-passage (P3) cultivation only. Never P4, never P5, never “just this once.”
- Up to 200 million cells within that P3 ceiling. Quantity within the youth window, not at its expense.
- If a case would require expansion beyond P3 to reach 200 million, we revise the plan. We do not release over-aged cells to hit a marketing number.
Many overseas clinics quietly deliver P5 or higher because it is cheaper and produces more batches per culture. The cells still “look like” stem cells under a microscope. They just do not work as well.
Question 2 — What Type of Stem Cells Should You Use?
Mesenchymal stem cells come from three main sources:
- Adipose (fat) tissue — your own, via a short mini-liposuction under local anesthesia
- Bone marrow — your own, via needle into the hip bone, often under general anesthesia
- Umbilical cord — a donor’s, collected at someone else’s birth
Cell Grand Clinic uses your own adipose (fat) cells — autologous ADSCs. The short version of why is on this page. The details are in the table below.

Why Autologous ADSC — The Three Things That Matter Most
1. Your own cells, so zero rejection and zero allergy. Because the cells are yours, your immune system recognizes them as self. That single fact removes three risks you cannot fully avoid with donor cells: allergic/hypersensitivity reactions, immune rejection, and disease transmission.
2. Easy, low-burden harvest. A 30-minute mini-liposuction under local anesthesia is all it takes. Most patients return to their hotel the same day — no hospitalization, no general anesthesia, no needle into the hip bone.
3. Adipose holds up with age, bone marrow doesn’t. A review in Cell Transplantation (https://doi.org/10.1177/0963689717721203) summarized it clearly: in older donors, bone marrow MSC quantity, proliferation, and osteogenic function all decline — but subcutaneous adipose tissue is largely unaffected by donor age, and the adipose secretome (the repair signals the cells actually release) is preserved. Proteomic work in Stem Cell Research & Therapy (https://doi.org/10.1186/s13287-020-02050-6) confirmed that adult-donor MSCs can still produce strong immunomodulatory signals when properly primed.
In plain language: if you are in your 50s, 60s, or 70s — which is when most people actually need stem cell therapy — adipose is the tissue that gives you the best shot at useful autologous treatment. And because the cells are yours, the biggest safety risks of donor cells simply do not apply.
| Factor | Autologous ADSC (Cell Grand) |
Allogeneic UC-MSC (Overseas) |
Autologous BM-MSC (Bone Marrow) |
|---|---|---|---|
| Cell source | Your own fat tissue | A donor’s umbilical cord | Your own bone marrow |
| Harvest method | Mini-liposuction · local anesthesia · ~30 min | Collected at someone else’s birth | Needle aspiration into hip bone · often general anesthesia |
| Allergy / rejection risk | Virtually zero (self) | Present — foreign cells can trigger immune reaction | Virtually zero (self) |
| Disease transmission | None (your own cells) | Possible if donor screening inadequate | None (your own cells) |
| Impact of your age | Identity and paracrine signaling preserved; proliferation slows | Not applicable (donor is a newborn) | Quantity, proliferation, and osteogenic function decline with age |
| Donor traceability | You are the donor — full chain of custody | Donor history often undisclosed; pooled batches possible | You are the donor — full chain of custody |
| Regulatory oversight | Japan MHLW Type II license · inspected CPC | Varies widely by country | Japan MHLW if Japan-based; varies elsewhere |
Question 3 — What Is the Right Amount? (Why More Is Not Always Better)
100–200 million cells per session is the evidence-backed high dose. Above that, you stop gaining benefit and start gaining risk.
Above 200 million cells in a single IV push, two things may happen:
- Efficacy stops scaling. A 2022 meta-analysis in Current Stem Cell Research & Therapy (https://doi.org/10.2174/1574888X16666210816111031) showed doses above 10⁸ cells produced a noisy +4.7% LVEF signal — but with extreme heterogeneity (I² = 95%) and confidence intervals crossing zero. The average “benefit” became statistically unreliable.
- Embolism risk goes up. A 2020 review in Frontiers in Immunology (https://doi.org/10.3389/fimmu.2020.01091) documented the mechanism: MSCs carry the procoagulant protein tissue factor (CD142) on their surface. When too many cells hit the lungs at once on the first IV pass, the risks include pulmonary microembolism, shortness of breath, hemodynamic instability, and thromboembolic events.
Cell Grand Clinic’s Ceiling
Cell Grand Clinic delivers up to 100 million cells per joint for intra-articular protocols and up to 200 million cells per session for systemic IV protocols — at the top of the evidence envelope, never above it. When a case needs more total exposure, we achieve it through planned, spaced sessions, not a reckless single push. Slower. Safer. Backed by the data.
10 Questions to Ask Any Stem Cell Clinic (Japan or Anywhere Else)
Use this list anywhere — in Japan, Mexico, Thailand, the U.S., or elsewhere. An evidence-based clinic should be able to answer every point in writing:
- Are the cells autologous or allogeneic? If allogeneic, how is donor screening documented?
- What tissue source? (adipose, bone marrow, umbilical cord)
- What is the final viability at the moment of administration? (Specific percentage, for this batch.)
- Have the cells been tested against the ISCT Dominici 2006 criteria? Which markers, what percentages?
- What passage number are the cells at? (P3? P5? P7+?)
- How many cells in total? Is the number based on what actually works, or what sounds impressive?
- Is the laboratory licensed by a national regulator — not just “GMP-like”?
- What adverse-event reporting system covers my treatment?
- Who are the named cultivation specialists, and how are they certified?
- Will I receive written documentation of the quality results for my specific batch?
At Cell Grand Clinic, every answer is documented — and signed off in the Certificate of Quality issued for each treatment.
Inside the Laboratory — Where Your Cells Come to Life
The laboratory matters as much as the clinic. Cell Grand Clinic cultivates each patient’s stem cells exclusively at an MHLW-licensed Cell Processing Center (License No. FA5250001) — a pharmaceutical-grade facility, not a commercial beauty lab.
| FACILITY CREDENTIAL MHLW Certified Cell Processing Facility License No. FA5250001 | GMP-Grade Cleanroom | 24/7 Monitoring | Robotics-Assisted Cultivation |
|---|

Academic Linkage — Joint Research With Prof. Takahiro Ochiya
Our partner CPC conducts joint research with Professor Takahiro Ochiya of Tokyo Medical University, one of the world’s most cited researchers in exosomes and extracellular vesicles — the very signaling molecules that carry much of the stem cell’s therapeutic effect. The scientific insight from his ongoing research feeds directly into the cultivation protocols used for your treatment. This academic linkage is rare in the clinic space and is a real quality differentiator, not a marketing flourish.
Pharmaceutical-Grade Cleanroom, Real-Time Monitoring
Cells are cultivated inside a Grade A cleanroom within a Grade B background environment, with Grade C and D support zones — the same air-purity classifications used to manufacture injectable drugs. Temperature, humidity, pressure differentials, and particle counts are recorded continuously, 24 hours a day, for full regulatory traceability.
Dedicated Specialists, Not Rotating Technicians
Every step — isolation, expansion, passage control, identity testing, viability check, release — is performed by full-time, aseptic-technique-certified specialists trained on Japan’s Regenerative Medicine Safety Act protocols. No outsourced hands. No rotating shifts. Your cells are not a side project for anyone.
End-to-End Traceability
From the moment your fat tissue leaves the clinic to the moment your cultured cells are delivered for administration, every parameter, every operator action, and every environmental reading is logged. If a single deviation is flagged at any stage, the batch is held for investigation before it can be released. This is the same discipline applied to manufacturing injectable drugs, because that is effectively what cell therapy is.

Why Japan — and Why Cell Grand Clinic
Japan is the only major nation with comprehensive legislation specifically for regenerative medicine: the Act on the Safety of Regenerative Medicine, enacted in 2014. The framework requires:
- Treatment plans reviewed and certified by an MHLW-accredited regenerative medicine committee before a single patient is treated
- Licensed Cell Processing Facilities under regular government inspection
- Mandatory adverse-event reporting into a national database
- Classification into Types I–III by risk level, with corresponding oversight
Cell Grand Clinic operates under 13 separate Regenerative Medicine Provision Plans accepted by Japan’s MHLW (Type 2 and Type 3, Plan No. PB5240089 and others) — one of the largest certified regenerative medicine portfolios of any single clinic in Japan. Each plan has been reviewed and approved by an MHLW-Certified Special Committee for Regenerative Medicine before a single patient can be treated under it. This is the legal infrastructure behind every Grand Stem Cell batch — not a voluntary self-claim.
The 13 certified plans cover the full range of age-related and quality-of-life conditions where adipose-derived stem cell therapy has the strongest evidence base:
- Musculoskeletal & pain — knee osteoarthritis · meniscus repair · chronic pain
- Metabolic & cardiovascular — type 2 diabetes · atherosclerosis · erectile dysfunction (often linked to vascular aging)
- Anti-aging / longevity — systemic anti-aging and “back-aging” protocols
- Aesthetic & dermatology — skin rejuvenation · hair loss (AGA / FAGA)
In other words, Cell Grand Clinic is not a single-indication boutique. It is a full-spectrum regenerative medicine clinic for the conditions that typically begin to matter in the second half of life — and every one of those indications is covered by a formally certified, government-reviewed treatment plan.
Medical direction is led by Yuichi Wakabayashi, M.D., Ph.D. — Diplomate of the American Board of Regenerative Medicine (ABRM), former NIH research fellow, first-author of the world’s first-in-human PDE4B-specific PET tracer study (with Pfizer Inc.), featured in the Wall Street Journal. With over 3,000 stem cell treatments performed, Dr. Wakabayashi personally reviews every international patient’s plan before treatment.
Frequently Asked Questions
I’m in my 60s. Are my own stem cells still worth using?
Yes. While cells from older donors proliferate more slowly in culture, published research shows subcutaneous adipose tissue and its stem cell secretome — the growth factors and signaling molecules responsible for repair — are largely preserved with age. Cell Grand Clinic’s P3 ceiling protects what matters most: the signaling quality of the cells you actually receive.
What does “passage 3 (P3)” mean and why does it matter?
A passage is one cycle of detaching, counting, and re-seeding cells. Each passage ages the cell a little. Research shows chromosomal abnormalities and loss of secretome activity rise sharply beyond passage 5. Cell Grand Clinic uses P3 cells only — a deliberate trade-off between having enough cells to treat and keeping those cells young enough to actually work.
How is “Grand Stem Cell” different from any other stem cell therapy?
Grand Stem Cell is Cell Grand Clinic’s internal quality standard that a batch must meet before release: made fresh for the individual patient, identity-verified against ISCT (Dominici 2006) criteria, ≥95% viability at administration, and cultivated only to passage 3. Every treated patient receives a Certificate of Quality documenting that their specific batch met all four pillars.
Is stem cell therapy completely safe?
No medical therapy is “completely” safe, and any clinic claiming otherwise should be treated with caution. Published clinical-trial data show mesenchymal stem cell therapy has a strong safety record when dose, viability, and identity are controlled, and when treatment occurs under regulatory oversight such as Japan’s Regenerative Medicine Safety Act. Risk profile varies by dose, route, and individual patient factors — an honest consultation will address all three.
Why does laboratory regulation matter so much?
Because stem cells are living therapeutic products, not sterile drugs you can quality-check at the end like a pill. Contamination, misidentification, or over-passaging can only be caught during cultivation — which is why a licensed, inspected, traceable Cell Processing Facility is not optional. The Grand Stem Cell standard is built on MHLW-licensed infrastructure for exactly this reason.
Can I see proof that my specific batch met quality standards?
Yes. Every patient at Cell Grand Clinic receives a Certificate of Quality documenting viability, surface-marker expression against ISCT criteria, final passage number, and total cell count for that individual batch. If any clinic — in any country — cannot give you this in writing for your specific treatment, treat that as your answer.
Closing — What You Are Actually Paying For
Stem cell therapy is not cheap. Nowhere in the world is it cheap when done properly. When you see a much lower price tag abroad, what is usually missing is not the cells themselves — it is everything around the cells:
- regulatory oversight that catches problems early
- identity testing so you know what is being infused
- viability verification so you know the cells are alive
- passage discipline so you know the cells are young
- dose discipline so you know the treatment fits the evidence
Grand Stem Cell is our way of guaranteeing, in writing, that none of these are skipped.
Updated: 2026.06.06