Inquiries by Email
Inquiries by Email
Stem cell therapy for erectile dysfunction uses mesenchymal stem cells to restore vascular and tissue function in the penis — for men seeking a drug-free alternative to PDE5 inhibitors and implants.
Below: How stem cells repair penile vasculature beyond PDE5 drugs, who qualifies, and how Japan’s MHLW oversight differs from offshore men’s clinics.
At Cell Grand Clinic in Osaka, Japan, cells cultured from your own minimal fat tissue over 7 weeks, never donor cells.
MHLW Type 2 certified. NIH-trained physician. 3,000+ cases.
- Living with ED — The Pill Cycle Many Men Want to End
- What Is Stem Cell Therapy for Erectile Dysfunction?
- Why Medication Alone Falls Short for Many Men
- How Stem Cell Therapy Restores Erectile Function
- Does Stem Cell Therapy Actually Work for ED?
- What About Diabetic ED and Peyronie’s Disease?
- Cell Grand Clinic’s Approach: Local Repair Plus Whole-Body Support
- Who Is a Good Candidate?
- The Treatment Process
- Possible Risks and Side Effects
- Stem Cell Therapy Pricing
- Why Japan — and Why Cell Grand Clinic?
- Ready to Stop Managing Symptoms and Start Repairing the Cause?
- Frequently Asked Questions
- Take the Next Step
- Ready to Stop Managing Symptoms and Start Repairing the Cause?
- References
Living with ED — The Pill Cycle Many Men Want to End
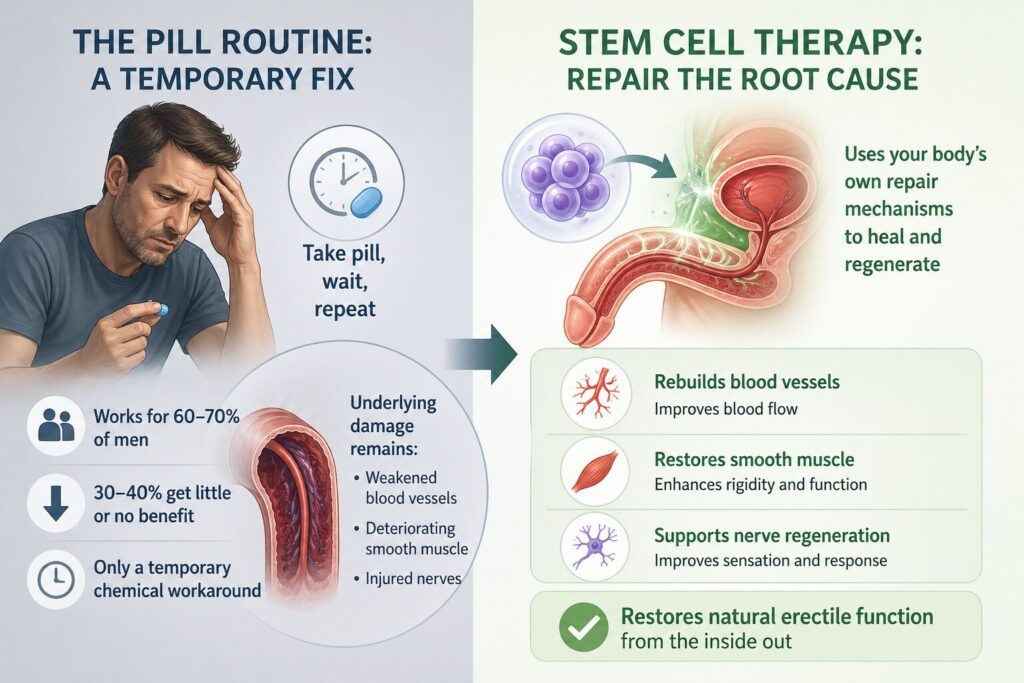
If you have been living with erectile dysfunction, you already know the routine. Take a pill, wait for it to work, hope the side effects are manageable — and repeat, every single time. For many men, this cycle becomes exhausting.
PDE5 inhibitors like Viagra and Cialis help roughly 60–70% of men — but that means 30–40% get little or no benefit at all. And even when the pills do work, they offer only a temporary chemical workaround. The moment the medication wears off, the underlying damage — weakened blood vessels, deteriorating smooth muscle, injured nerves — remains exactly where it was.
This is why a growing number of men are asking a different question: Is there a treatment that actually repairs erectile tissue, rather than masking the problem every few hours?
Stem cell therapy for erectile dysfunction is a regenerative medicine approach that uses the body’s own repair mechanisms to address the root causes of ED — rebuilding blood vessels, restoring smooth muscle, and supporting nerve regeneration. Rather than bypassing the problem with a pill, it aims to restore natural erectile function from the inside out.
What Is Stem Cell Therapy for Erectile Dysfunction?
Stem cell therapy for erectile dysfunction is a regenerative procedure that delivers mesenchymal stem cells — typically harvested from a patient’s own fat tissue — into the penile tissue and bloodstream to support repair of the vascular, muscular, and neural damage that contributes to ED.
Erectile dysfunction is far more than an inconvenience. It affects an estimated 322 million men globally, a number expected to climb as rates of diabetes, cardiovascular disease, and obesity continue to rise. While PDE5 inhibitors remain the first-line treatment, they work by temporarily blocking a single enzyme to increase blood flow for a few hours — they do not repair damaged tissue.
For men whose ED is driven by diabetes-related nerve and vascular damage, post-surgical nerve injury, Peyronie’s disease, or progressive age-related tissue degradation, medication alone often falls short. This is the gap that regenerative medicine aims to fill — not by masking the symptom, but by targeting the biological damage at its source.
Why Medication Alone Falls Short for Many Men
An erection requires precise coordination between the brain, nervous system, blood vessels, and penile smooth muscle. When a man becomes aroused, nerve signals trigger the release of nitric oxide, which relaxes smooth muscle in the corpora cavernosa, allowing blood to flow in and create rigidity. ED occurs when this chain is disrupted through one or more of four root mechanisms:
1. Endothelial damage — The inner lining of blood vessels deteriorates due to diabetes, hypertension, or smoking, reducing nitric oxide production.
2. Smooth muscle atrophy — The muscle within the corpora cavernosa loses mass and contractile function with age and disease, weakening the ability to trap blood.
3. Fibrosis — Collagen-rich scar tissue replaces healthy erectile tissue, reducing elasticity. In Peyronie’s disease, this causes visible curvature and functional impairment.
4. Nerve injury — The cavernous nerves that initiate erection can be damaged by diabetic neuropathy, radical prostatectomy, or pelvic radiation.
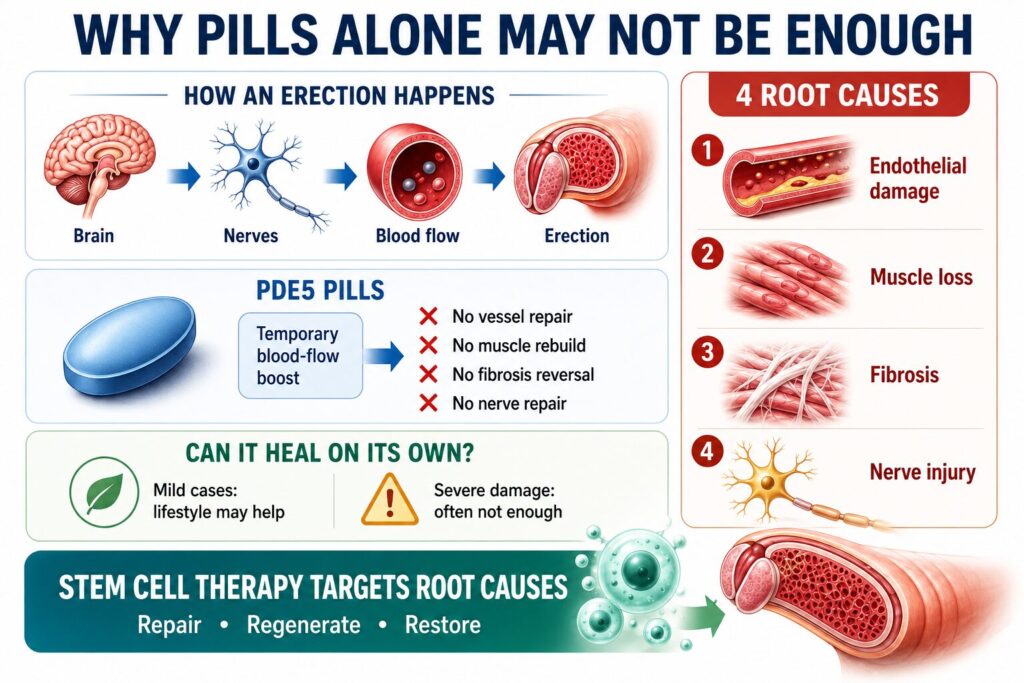
PDE5 inhibitors address only one of these four pathways — temporary blood flow enhancement — and only for a few hours at a time. They cannot repair endothelial cells, rebuild smooth muscle, dissolve fibrotic tissue, or regenerate nerves.
Can erectile tissue heal on its own? In mild cases with lifestyle changes, some limited natural recovery is possible. But when the underlying damage is significant — from diabetes, surgery, or years of progressive decline — the body lacks sufficient regenerative capacity to reverse it without intervention. This is precisely where stem cell therapy offers a fundamentally different approach.
How Stem Cell Therapy Restores Erectile Function
Mesenchymal stem cells (MSCs) support erectile function primarily through what researchers call the paracrine effect: once delivered to damaged tissue, these cells release a mix of growth factors and signaling molecules that activate the body’s own repair systems.
- New Blood Vessels — VEGF stimulates angiogenesis, supporting blood flow to erectile tissue
- Smooth Muscle Repair — bFGF promotes smooth muscle cell proliferation
- Nerve Regeneration — NGF and BDNF support cavernous nerve repair, especially relevant for men with post-surgical or diabetic nerve damage
- Anti-Fibrotic Action — HGF helps inhibit fibrosis and may support breakdown of existing scar tissue
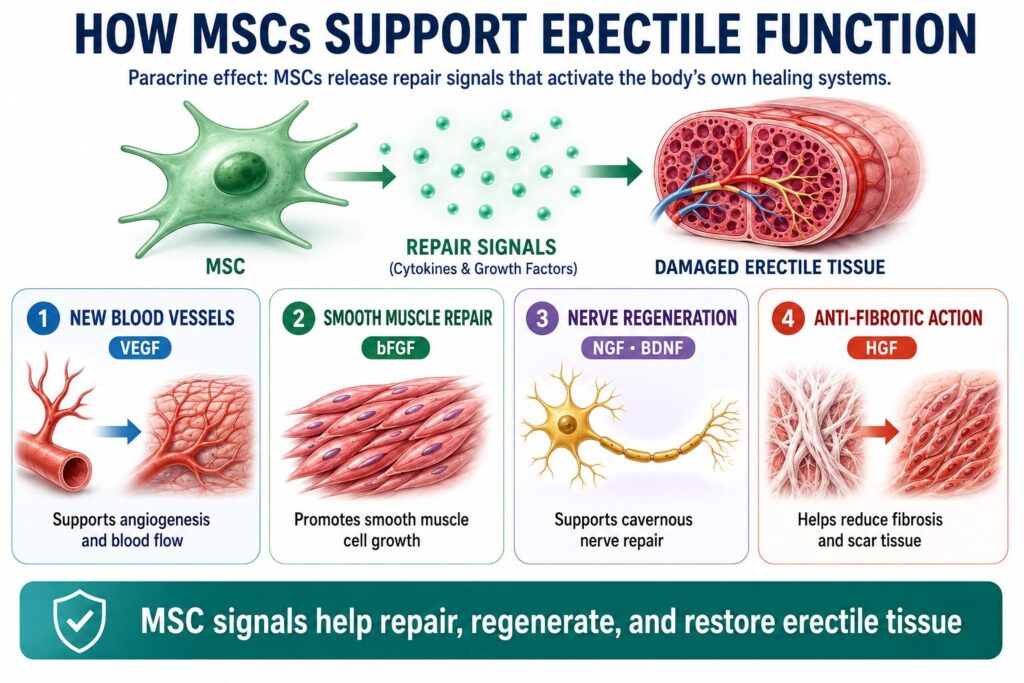
Unlike a medication that targets a single enzyme for a few hours, stem cells release many bioactive molecules — addressing multiple damage pathways at once and triggering biological processes that continue for weeks to months after treatment.
Adipose-derived stem cells (ADSCs) — the type used in this treatment — are harvested from a patient’s own fat tissue. Fat is a particularly accessible source of mesenchymal stem cells, with cell yields per gram of tissue substantially higher than bone marrow.² Because the cells come from the patient’s own body, there is no risk of allogeneic immune rejection, and no immunosuppressive medication is required.
A 2025 review published in Frontiers in Medicine (Fu et al., DOI) summarized the current state of stem cell research for ED, noting that both preclinical evidence and emerging clinical data support the regenerative potential of stem cells — particularly through paracrine-mediated vascular repair, smooth muscle support, and nerve growth factor secretion. The authors emphasize that this remains an area of active investigation.
Does Stem Cell Therapy Actually Work for ED?
Across published clinical trials, men who received stem cell injections for erectile dysfunction saw measurable improvement in erectile function — and no serious adverse events have been reported in any published study to date.
The most cited result comes from a Phase I trial in post-prostatectomy ED (Haahr et al., 2016, EBioMedicine):
73% of patients who retained urinary continence regained erections sufficient for intercourse at 6 months — from a single stem cell injection.
Translated into score terms: the IIEF-5 score in these patients improved from a baseline median of 7 (severe ED — rarely able to achieve erection sufficient for intercourse) to 17 (mild ED — usually able to complete intercourse) at 6 months. A 12-month follow-up confirmed sustained recovery in 53% of these men without any further treatment.
Two 2024–2025 meta-analyses pooling data across multiple trials confirmed statistically meaningful improvements in standardized erectile-function scores and penile blood flow.
Important: Stem cell therapy for ED is still an emerging treatment. Most published trials are small Phase I/II studies, and individual response varies depending on the cause and severity of ED, age, and overall health. Larger randomized trials are ongoing.
What About Diabetic ED and Peyronie’s Disease?
Two conditions are particularly common among the international patients we treat — and both have been studied specifically in published clinical trials.
Diabetic ED
Diabetic ED is one of the most studied populations in this field. Several trials, including the only randomized controlled trial published to date (Mirzaei et al., 2024), have reported improvement in erectile function in diabetic men who had stopped responding to PDE5 inhibitors.
In Mirzaei’s RCT, IIEF-5 scores rose by an average of 3.4 points in men receiving a single stem cell injection, versus essentially no change in the placebo group at 6 months — a clinically meaningful shift for patients who had been told there was “nothing more to try” after pills.
This matters because diabetic men respond poorly to PDE5 inhibitors compared with the general ED population, and they often have the kind of vascular and nerve damage that regenerative therapy is specifically designed to address.
Peyronie’s Disease
Peyronie’s disease — fibrotic plaques in the penile tunica that cause curvature, painful erections, and often ED — has been studied in only one published human stem cell trial (Levy et al., 2015, n=5). The numbers were striking:
7 of 10 fibrotic plaques completely disappeared at 3 months following stem cell injection, alongside improved penile blood flow.
Larger trials of platelet-rich plasma (PRP) — a related regenerative therapy — have shown reductions in penile curvature of 10 to 17 degrees without serious side effects.
Because the human stem cell evidence base for Peyronie’s disease is still small, treatment suitability is determined case by case, with particular attention to disease phase (active vs. chronic) and plaque characteristics (size, location, calcification). Active-phase patients — those still experiencing pain or progressive curvature — generally respond better than long-standing chronic plaques.
Cell Grand Clinic’s Approach: Local Repair Plus Whole-Body Support
Most published trials use a single intracavernous injection. Our standard ED protocol goes further, treating both the erectile tissue and the underlying body-wide conditions that drive ED in the first place:
- 50 to 100 million autologous adipose-derived stem cells (ADSCs) delivered directly into the erectile tissue (intracavernous injection) — to support local repair of blood vessels, smooth muscle, and nerves
- Intravenous (IV) infusion of additional autologous stem cells — to address the systemic factors behind ED: vascular endothelial dysfunction, chronic low-grade inflammation, diabetes, and metabolic dysregulation
ED is rarely a purely local problem. By treating both the penis itself and the systemic factors behind it, this combined approach is designed to give the regenerative process the best possible foundation for durable improvement.
Who Is a Good Candidate?
Stem cell therapy for erectile dysfunction may be particularly beneficial for men whose ED has not responded adequately to conventional treatment, or who seek a drug-free alternative that addresses the underlying cause.
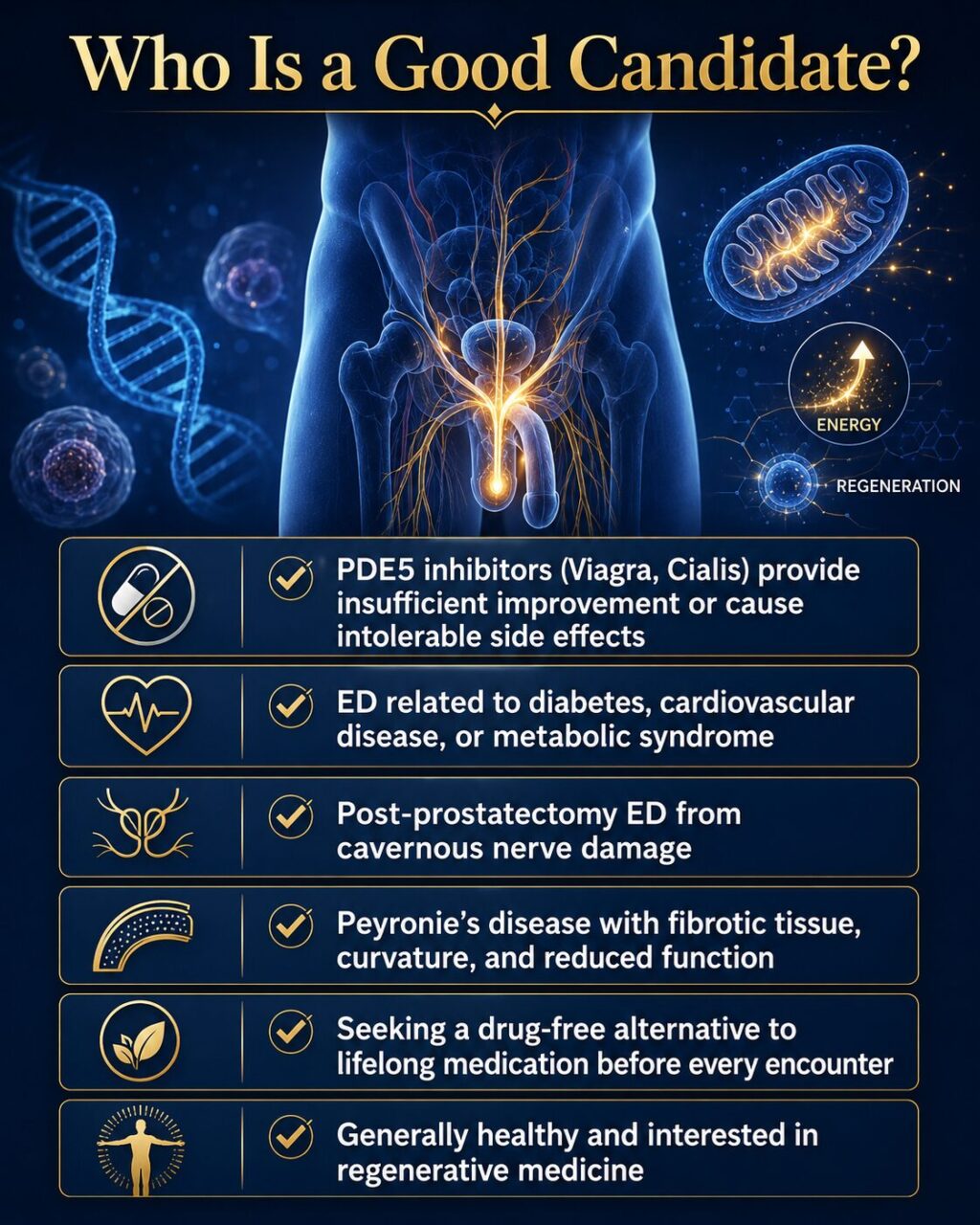
You may be a candidate if:
- ✓ PDE5 inhibitors (Viagra, Cialis) provide insufficient improvement or cause intolerable side effects
- ✓ Your ED is related to diabetes, cardiovascular disease, or metabolic syndrome
- ✓ You have post-prostatectomy ED from cavernous nerve damage
- ✓ You have Peyronie’s disease with fibrotic tissue causing curvature and reduced function
- ✓ You want a drug-free alternative to lifelong reliance on medication before every encounter
- ✓ You are generally healthy and interested in regenerative medicine as part of a proactive health strategy
Individual suitability is determined during a medical consultation. This checklist is for general reference only.
Stem Cell Therapy for Diabetes: A Regenerative Approach to Glycemic Control Learn More Improving Atherosclerosis: Stem Cell Therapy for Vascular & Cardiac Health Learn MoreThe Treatment Process
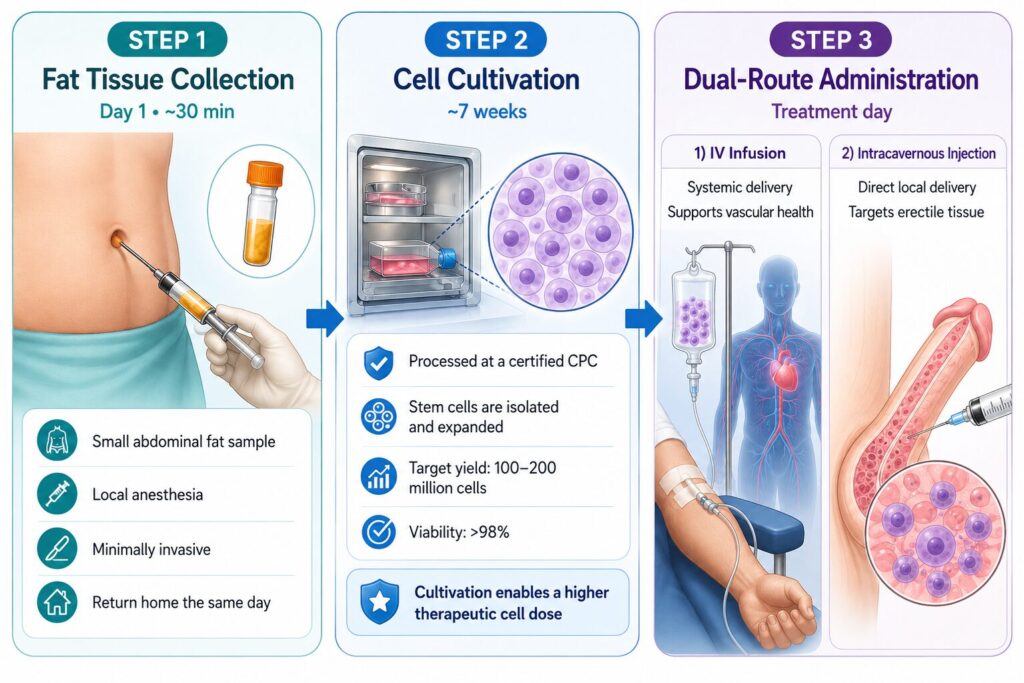
Step 1 — Fat Tissue Collection (Day 1, approximately 30 minutes)
A small amount of fat tissue — roughly 10 milliliters — is collected from the abdomen under local anesthesia. The procedure is minimally invasive and comparable in discomfort to a standard blood draw. You can return to normal activities the same day.
On the very same day as your fat collection, you also have the option to receive exosome therapy. Culturing your own stem cells takes several weeks, and many patients don’t want to simply wait while their symptoms continue. Exosomes—the tiny signaling messengers naturally released by stem cells—can help calm inflammation and ease discomfort during this period, so you’re already starting to feel better by the time your cultured cells are ready. Think of it as a bridge: exosomes work with your treatment timeline, not against it.
Step 2 — Cell Cultivation (Approximately 7 Weeks)
Your harvested tissue is sent to a government-certified Cell Processing Center (CPC), where stem cells are isolated and expanded under strict pharmaceutical-grade conditions. Over approximately seven weeks, cells are grown to reach a therapeutic dose of 100 to 200 million viable stem cells with a verified viability rate above 98%.
This extended cultivation period is critical. Some clinics offer same-day procedures using uncultured cells — often yielding only a few million cells. The difference in therapeutic dose is substantial.
Step 3 — Dual-Route Administration (Treatment Day)
Intracavernous injection concentrates cells directly into the penile erectile tissue, supporting local regenerative signaling where tissue damage is most severe.
Intravenous (IV) infusion delivers stem cells systemically, targeting the cardiovascular inflammation and endothelial dysfunction that often underlie ED.
Exosome Therapy: Same-Day, Cell-Free Regeneration Learn MoreRecovery Timeline
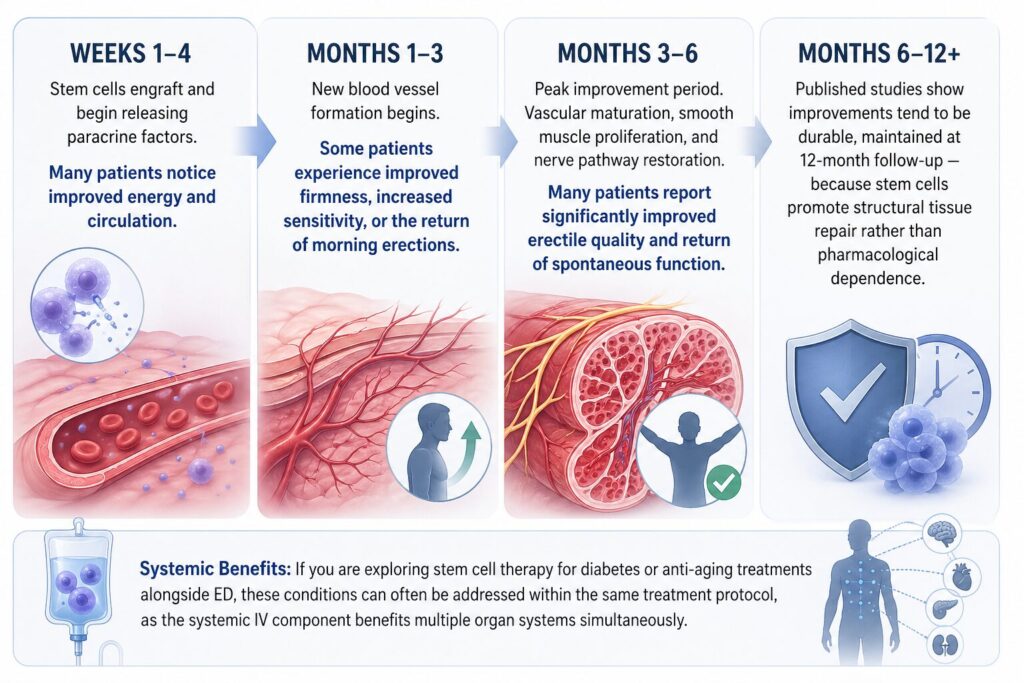
Weeks 1–4: Stem cells engraft and begin releasing paracrine factors. Many patients notice improved energy and circulation.
Months 1–3: New blood vessel formation begins. Some patients experience improved firmness, increased sensitivity, or the return of morning erections.
Months 3–6: Peak improvement period. Vascular maturation, smooth muscle proliferation, and nerve pathway restoration. Many patients report significantly improved erectile quality and return of spontaneous function.
Months 6–12+: Published studies show improvements tend to be durable, maintained at 12-month follow-up — because stem cells promote structural tissue repair rather than pharmacological dependence.
If you are exploring stem cell therapy for diabetes or anti-aging treatments alongside ED, these conditions can often be addressed within the same treatment protocol, as the systemic IV component benefits multiple organ systems simultaneously.
Reverse Aging: How Stem Cell IV Therapy Actually Works Learn HowPossible Risks and Side Effects
Like any medical procedure, stem cell therapy for ED carries risks that should be understood before deciding to proceed. Across published clinical trials, no serious adverse events have been reported, and the safety profile is favorable — but minor and theoretical risks exist:
Common minor side effects (typically resolve within 1–2 weeks):
- Temporary swelling, mild bruising, or tenderness at the injection site
- Mild discomfort at the liposuction site (small abdominal area)
- Brief soreness during or after the IV infusion
Less common but possible:
- Local hematoma at the penile injection site (managed with compression and observation)
- Mild infection at the liposuction or injection site (managed with antibiotics if it occurs)
- Transient elevation of inflammatory markers in blood tests
Theoretical risks discussed in the regenerative medicine literature:
- Long-term safety data beyond 5 years remains limited; the longest published follow-up periods in the literature have not reported safety concerns
- As with any cell therapy, theoretical immune or proliferative concerns are part of ongoing scientific monitoring
Because all cells used at Cell Grand Clinic are autologous (your own), there is no risk of allogeneic immune rejection or graft-versus-host disease — risks that can occur with donor-derived cell therapies.
All risks are reviewed in detail during your medical consultation, and informed consent is obtained before any procedure.
Stem Cell Therapy Pricing
$19,800 USD includes:
- 100 million autologous ADSCs
- 7-week culture at MHLW-certified CPC
- Quality certificate · 98%+ viability
- 6 + 12 month remote follow-up
Final pricing depends on your individual case:
- Higher cell counts (200 million+)
- Combination protocols
- Multiple sessions
Why Japan — and Why Cell Grand Clinic?
Japan’s Regenerative Medicine Regulatory Framework
Japan is one of the only countries with a comprehensive legal framework specifically designed for regenerative medicine. The Act on the Safety of Regenerative Medicine (enacted 2013, amended 2020) requires every stem cell treatment plan to be reviewed and approved by an independent MHLW-Certified Special Committee before it can be offered to patients.
This is not self-regulation — it is government-mandated oversight with real accountability. Every treatment protocol, every cell processing step, and every safety measure is documented and monitored.
| Factor | Japan (MHLW-certified) | Mexico | Thailand |
|---|---|---|---|
| Government Oversight | MHLW certified ✓ | Limited regulation | Emerging regulation |
| Cell Quality Standards | CPC-grade, 7-week culture ✓ | Varies by clinic | Varies by clinic |
| Cell Count per Treatment | Up to 200 million ✓ | Varies widely | Varies widely |
| Autologous (Own Cells) | Yes ✓ | Often allogeneic | Mixed |
| Physician Credentials | NIH-trained, ABRM Diplomate ✓ | Varies | Varies |
Comparison is based on general regulatory frameworks. Individual clinics may vary. Japan’s MHLW certification system (Act on the Safety of Regenerative Medicine) is unique in providing government-level oversight for regenerative treatments.
Cell Grand Clinic: What Sets Us Apart
Cell Grand Clinic operates under Japan’s Act on the Safety of Regenerative Medicine, holding 13 government-approved treatment plans — among the highest numbers of any regenerative medicine clinic in Japan (Plan No. PB5240089 and others).
Cell Grand Clinic is directed by Dr. Yuichi Wakabayashi, M.D., Ph.D., a Diplomate of the American Board of Regenerative Medicine (ABRM) with research experience at the U.S. National Institutes of Health (NIH). With over 3,000 stem cell treatments performed, Dr. Wakabayashi brings international research credentials and clinical experience to every patient’s treatment plan.
Cell quality is central to our approach. Every batch is cultivated for approximately 7 weeks at a certified CPC, tested for viability (98%+), screened for infectious agents, and accompanied by a certificate of quality. Cell Grand Clinic does not use frozen, pre-made, or off-the-shelf cell products.
Cell Quality: The Key Factor That Impacts Stem Cell Therapy Outcomes Learn MoreReady to Stop Managing Symptoms and Start Repairing the Cause?
If you have spent years cycling through pills, injections, or vacuum devices — only to watch the underlying problem get worse — you have probably already done your research. You know the studies. You have read the meta-analyses. The question now is: does your specific case qualify, and what would it actually cost?
Here is how to find out without committing to anything:
- Send your case via WhatsApp or email — medical history, current treatments, what is not working
- Dr. Wakabayashi reviews it personally — not delegated to a coordinator
- Get a written response within 24 hours with feasibility, treatment timeline, and price quote
- Decide on your timeline — most international patients schedule treatment 4–8 weeks after their first inquiry to allow for travel planning
Frequently Asked Questions
Can stem cells repair erectile dysfunction?
Early clinical evidence suggests stem cell therapy may improve erectile function by supporting repair of damaged blood vessels, smooth muscle, and nerves. A 2025 meta-analysis (Senel et al.) found significant improvements in erectile function scores at six months. However, results vary by individual, and stem cell therapy for ED is still classified as an emerging treatment. Larger trials are underway to establish long-term efficacy.
How much does stem cell therapy for erectile dysfunction cost?
In Japan, autologous stem cell therapy for ED typically costs approximately $19,800 USD per session, depending on cell count, cultivation protocol, and administration method. This is not covered by insurance. Pricing varies by individual case — contact Cell Grand Clinic for a personalized estimate.
How long does stem cell therapy for ED take to work?
Most patients begin noticing initial changes within one to three months, with peak effects in published studies typically occurring between three and six months after treatment. Because stem cells work through tissue support rather than pharmacological effect, the process is gradual. Published studies show benefits often maintained at 12-month follow-up (e.g., Haahr 2018: 53% sustained recovery), though individual durability varies.
Is stem cell therapy for ED safe?
Across published clinical trials of intracavernous stem cell injection for ED, no serious adverse events have been reported. Side effects are limited to mild, temporary swelling or bruising at the injection site. Because Cell Grand Clinic uses autologous (your own) cells, there is no risk of allogeneic immune rejection.
What is the success rate of stem cell therapy for ED?
Success rates vary by study and patient population. In the Haahr et al. 2016 trial (using freshly isolated ADRC/SVF), 47% of men with severe post-prostatectomy ED recovered function after a single injection at 6 months — and 73% among continent patients. The 12-month follow-up (Haahr 2018) showed 53% sustained recovery in continent patients. A 2023 systematic review of 18 clinical studies involving 373 patients found consistent safety and efficacy signals across multiple stem cell types. Individual results depend on the cause and severity of ED, and outcomes cannot be predicted in advance.
Can stem cells cure erectile dysfunction permanently?
No treatment can guarantee a permanent cure, and it would be inaccurate to claim otherwise. Stem cell therapy aims to produce durable improvement by supporting underlying tissue repair, but durability varies between patients. Published trials show some sustained benefits at 12+ months in responders, while some patients may require additional sessions.
Can erectile tissue heal on its own?
In mild cases, lifestyle changes such as improved diet, exercise, and managing conditions like diabetes can support some natural recovery. However, when significant structural damage exists — from disease, surgery, or years of progressive decline — the body’s natural repair capacity is often insufficient. Stem cell therapy may provide additional regenerative support beyond what damaged erectile tissue can generate on its own.
Can stem cells increase size?
Stem cell therapy for ED is designed to support natural erectile function — not to increase penile size. The treatment works by supporting tissue repair and blood flow, which may result in firmer, fuller erections closer to a patient’s natural baseline. Claims about permanent size increase from stem cells are not supported by current clinical evidence.
Is stem cell therapy for ED approved by the FDA or Japan’s MHLW?
In the United States, the FDA has not approved stem cell therapy for ED. In Japan, stem cell therapy operates under a different legal framework: the Act on the Safety of Regenerative Medicine, which requires government-certified committee review of every treatment plan. Cell Grand Clinic’s treatment plans have passed this review process. This is distinct from “FDA approval” — it provides regulated safety oversight, not an efficacy guarantee.
Does stem cell therapy work for ED after prostatectomy?
The Haahr et al. 2016 Phase I trial enrolled 17 men with post-prostatectomy ED who had failed PDE5 inhibitor treatment, using freshly isolated adipose-derived regenerative cells (ADRC/SVF). At 6 months, 73% of continent patients (8 of 11) recovered erectile function sufficient for intercourse. The 12-month follow-up (Haahr 2018, n=21) reported 53% sustained recovery in continent patients. Cavernous nerve repair support is one of the proposed mechanisms by which stem cell therapy may help recovery after prostate surgery, though individual results vary.
Take the Next Step
Erectile dysfunction is not something you simply have to accept. It is a medical condition with identifiable biological causes — and regenerative medicine offers a genuine pathway to address those causes rather than masking them with medication.
If PDE5 inhibitors have not worked for you, if your ED is driven by diabetes, surgery, or progressive vascular disease, or if you want an evidence-based, drug-free approach to restoring your sexual health — we invite you to explore what stem cell therapy at Cell Grand Clinic can offer.
Ready to Stop Managing Symptoms and Start Repairing the Cause?
If you have spent years cycling through pills, injections, or vacuum devices — only to watch the underlying problem get worse — you have probably already done your research. You know the studies. You have read the meta-analyses. The question now is: does your specific case qualify, and what would it actually cost?
Here is how to find out without committing to anything:
- Send your case via WhatsApp or email — medical history, current treatments, what is not working
- Dr. Wakabayashi reviews it personally — not delegated to a coordinator
- Get a written response within 24 hours with feasibility, treatment timeline, and price quote
- Decide on your timeline — most international patients schedule treatment 4–8 weeks after their first inquiry to allow for travel planning
References
Senel S, et al. Stem cell therapy for erectile dysfunction: promise or reality? — a systematic review and meta-analysis of clinical trials. BMC Urol. 2025;25(1):222. https://doi.org/10.1186/s12894-025-01913-5
Hinojosa-Gonzalez DE, et al. Regenerative therapies for erectile dysfunction: a systematic review, Bayesian network meta-analysis, and meta-regression. J Sex Med. 2024;21(12):1152-1158. https://doi.org/10.1093/jsxmed/qdae131
Furtado TP, et al. Stem cell therapy for erectile dysfunction: a systematic review. Sex Med Rev. 2023;12(1):87-93. https://doi.org/10.1093/sxmrev/qead040
Ji YH, et al. High-activity placenta-derived mesenchymal stem cells combined with low-intensity extracorporeal shock wave therapy for diabetic erectile dysfunction: a prospective randomized controlled trial. Stem Cell Res Ther. 2025;16(1):359. https://doi.org/10.1186/s13287-025-04499-9
Haahr MK, et al. Safety and potential effect of a single intracavernous injection of autologous adipose-derived regenerative cells in patients with erectile dysfunction following radical prostatectomy: an open-label phase I clinical trial. EBioMedicine. 2016;5:204-210. https://doi.org/10.1016/j.ebiom.2016.01.024
Nguyen Thanh L, et al. Can autologous adipose-derived mesenchymal stem cell transplantation improve sexual function in people with sexual functional deficiency? Stem Cell Rev Rep. 2021;17(6):2153-2163. DOI
Al Demour S, et al. Safety and efficacy of 2 intracavernous injections of allogeneic Wharton’s jelly-derived mesenchymal stem cells in diabetic patients with erectile dysfunction: Phase 1/2 clinical trial. Urol Int. 2021;105(11-12):935-943. https://doi.org/10.1159/000517364
Fu X, et al. Advances in stem cell therapy for erectile dysfunction: preclinical evidence and emerging therapeutic approaches. Front Med. 2025;12:1519095. https://doi.org/10.3389/fmed.2025.1519095
Updated: 2026.06.06