Inquiries by Email
Inquiries by Email
Stem cell therapy for knees is the intra-articular injection of adipose-derived mesenchymal stem cells (ADSCs) to treat knee osteoarthritis — designed for patients with Kellgren-Lawrence Grade I-III disease who want a non-surgical, biologically active alternative.
Below: how four cellular mechanisms repair cartilage, what 2025 meta-analytic evidence shows by KL grade, and why Japan’s MHLW-regulated protocol differs from donor stock cells in Mexico, Panama, and Cayman.
At Cell Grand Clinic in Osaka, Japan, cells cultured from your own minimal fat tissue over 7 weeks — up to 100 million autologous cells via intra-articular injection, never donor.
- What Is Stem Cell Therapy for Knees and Knee Osteoarthritis?
- When Conservative Care Stops Working — Beyond NSAIDs, HA, and Cortisone
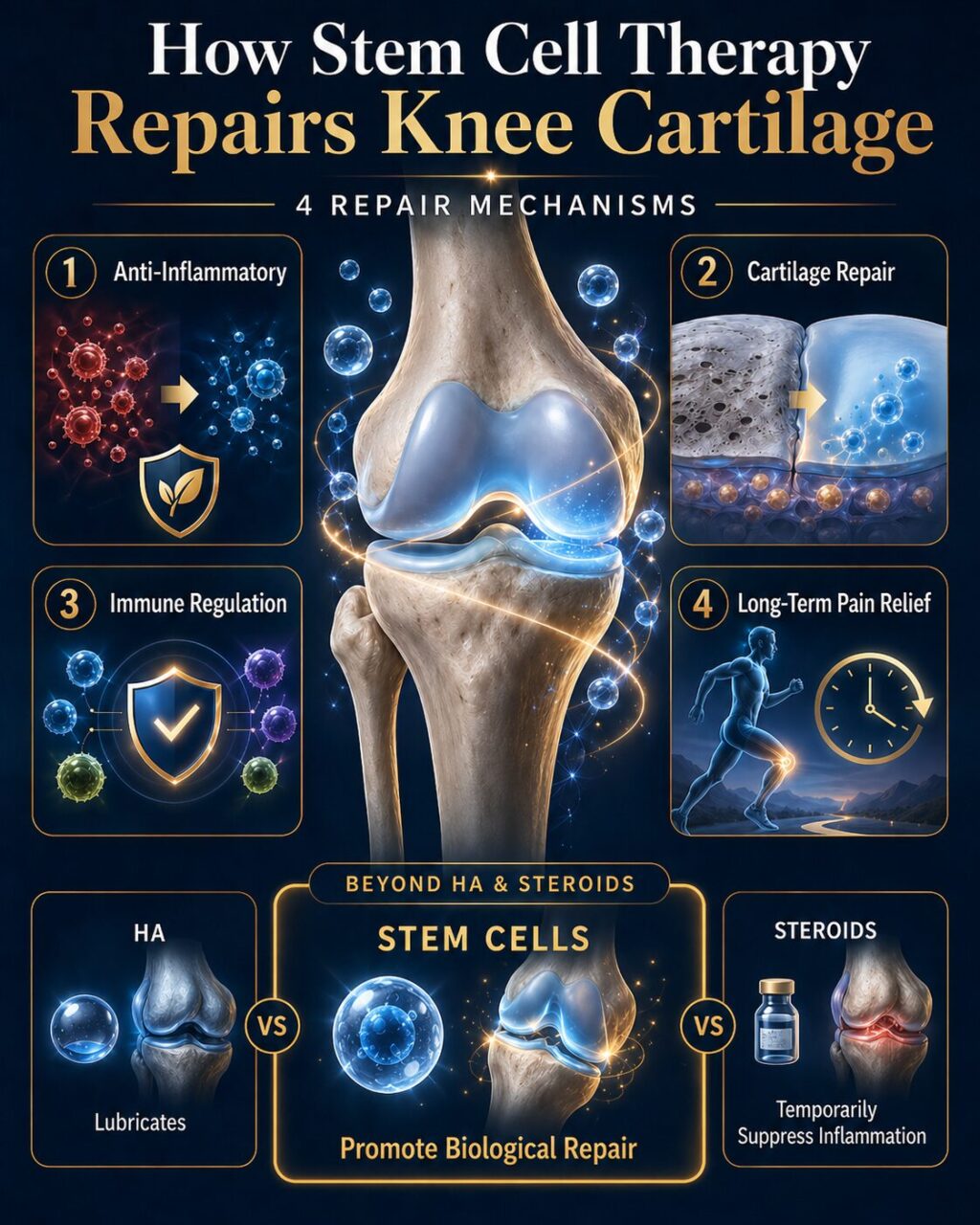
- How Stem Cells Repair Knee Cartilage — The 4 Mechanisms
- Does Stem Cell Therapy Work for Knees? The 2025 Meta-Analytic Evidence
- Outcomes by Kellgren-Lawrence Grade — I, II, III, and IV
- How Many Stem Cells Do You Need? Why 100 Million Is the Threshold
- ADSC vs BMAC vs Donor Stock Cells — Why Adipose Outperforms for Knees
- Why Autologous in Japan, Not Donor Stock from Mexico or Cayman
- Cell Grand Clinic — Grand Stem Cell, ABRM Physician, 3,000+ Cases
- Knee Stem Cell Treatment Process
- Who Is a Candidate, and What Are the Pros and Cons?
- Postpone the knee replacement — repair the cartilage first.
- Frequently Asked Questions
- Conclusion: Restore Your Mobility — Naturally
- References
What Is Stem Cell Therapy for Knees and Knee Osteoarthritis?
Knee osteoarthritis is the gradual breakdown of the protective cartilage covering the ends of the femur and tibia, with thickening of underlying bone, inflammation of the joint lining, and progressive pain, stiffness, and loss of motion. Approximately 240 million people worldwide live with this disease, and 33% of adults over the age of 75 have both symptomatic and radiographic knee osteoarthritis, as documented in the 2021 review published in JAMA (Katz, Arant, and Loeser 2021).
The goal of stem cell therapy is biological disease modification at the joint level, not only symptom suppression. Unlike hyaluronic acid (which lubricates) or PRP (which delivers growth factors for several days), stem cells continuously release a cocktail of anti-inflammatory cytokines and trophic growth factors for weeks — which is why they sit on a different shelf of the treatment ladder.
A 2025 meta-analysis of 502 patients across 8 randomized controlled trials, published in Stem Cell Research & Therapy (Cao, Ou, Sheng et al. 2025), confirmed that intra-articular MSC injection alone — without surgery — significantly improves WOMAC pain and function scores at both 6 and 12 months. The treatment is appropriate for Kellgren-Lawrence Grade I-III osteoarthritis, with strongest evidence in Grade II-III. For Grade IV bone-on-bone disease, stem cells can offer meaningful pain relief but cannot rebuild a structurally collapsed joint.
When Conservative Care Stops Working — Beyond NSAIDs, HA, and Cortisone
You have probably worked through the conservative ladder already. NSAIDs help, but five years of daily use shows up in your kidneys and stomach. Hyaluronic acid felt useful for a year, then noticeably less. Steroid shots clear the flare but cannot be repeated frequently. Your orthopedist mentions a total knee replacement (TKA), but you are 60, you travel, you ski, and 6–12 weeks of recovery plus a 15-year implant lifespan are not the answer you wanted.
This is exactly the gap that stem cell therapy occupies — between symptom management that has plateaued and a major operation that may be overkill. The 2025 Cao meta-analysis confirmed not only short-term pain reduction (6-month WOMAC MD=7.44, P=0.01) but durable function improvement at 12 months (MD=10.31, P=0.03), with adipose-derived cells outperforming bone-marrow cells. That durability is what NSAIDs and HA cannot offer.
Stem cell therapy is not a guarantee, and it is not for everyone. But for the right patient — early to moderate disease, motivated, willing to fly to Japan twice over 10 weeks — it is the most evidence-supported non-surgical option available today.
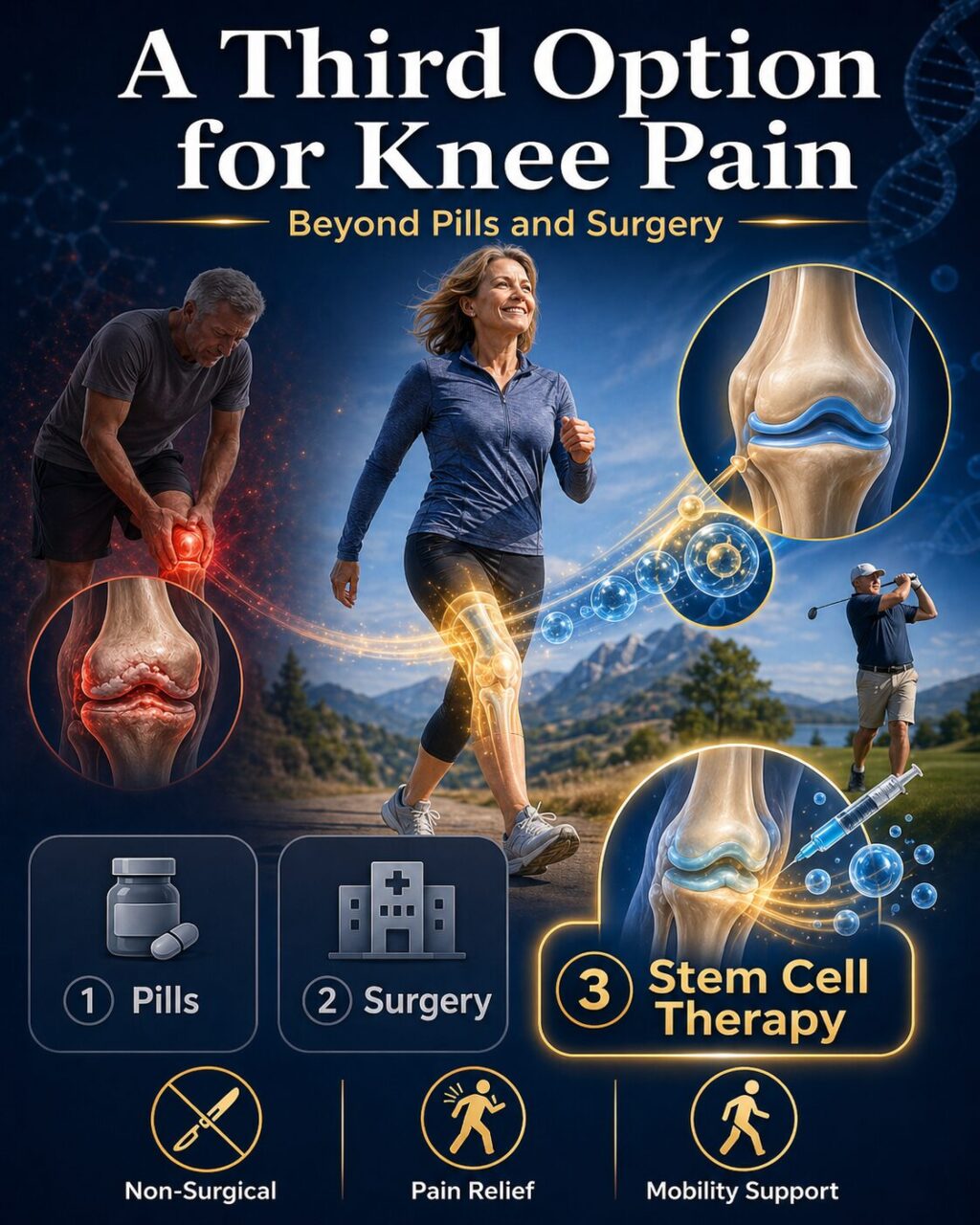
Doctors classify knee OA severity using the Kellgren-Lawrence (KL) system based on X-ray findings:
Stem cell therapy achieves the best outcomes for patients with KL Grade II–III OA, where sufficient cartilage remains for the stem cells to support repair. Even some Grade IV patients experience meaningful pain relief.
Alternatives to Knee Replacement: PRP, HA, MSC & Exosome Compared Compare OptionsHow Stem Cells Repair Knee Cartilage — The 4 Mechanisms
Understanding why stem cells do something a drug cannot helps you set realistic expectations. The four mechanisms below are documented in mechanistic reviews and clinical trials.
Anti-Inflammatory Action — Calming Joint Inflammation
The first mechanism is the rapid suppression of joint inflammation. Mesenchymal stem cells secrete anti-inflammatory cytokines including IL-10, TGF-β, and PGE2, which quiet the pro-inflammatory cascade driving osteoarthritis pain. This effect begins within days and is sustained for weeks, as detailed in the 2020 mechanistic review published in Trends in Pharmacological Sciences (Song, Scholtemeijer, and Shah 2020).
Cartilage Protection and Repair — Regenerative Signaling
The second mechanism is cartilage protection and regenerative signaling. MSCs release trophic factors that support chondrocyte (cartilage cell) survival and stimulate matrix production, while reducing the catabolic enzymes (MMPs, aggrecanases) that degrade cartilage. A 2023 review of 26 clinical studies (15 RCTs plus 11 non-RCTs, totaling 610 patients) published in Cellular & Molecular Immunology (Copp, Robb, and Viswanathan 2023) documented cartilage protection or repair in 18 of 21 clinical studies. Stem cells do not rebuild a fully collapsed joint, but they preserve and modestly regenerate cartilage thickness in early-to-moderate disease.
Immune System Regulation — Long-Term Joint Homeostasis
The third mechanism is immune modulation — MSCs reprogram the local joint immune environment from a pro-inflammatory state to a homeostatic one. This explains the durability of effect: even after the injected cells are cleared, the local immune landscape remains better regulated for months, per the same 2023 Copp et al. analysis.
Sustained Pain Relief — 12+ Months Documented
The fourth mechanism is the sustained downstream effect on pain. The 2025 Cao meta-analysis confirmed significant WOMAC pain score improvement at both 6 and 12 months. A separate 5-year follow-up study published in Stem Cells Translational Medicine (Kim, Lee, Kim et al. 2022) demonstrated that a single intra-articular high-dose (1×10⁸ cells) autologous ADMSC injection provided pain and functional improvement maintained for 5 years.
Does Stem Cell Therapy Work for Knees? The 2025 Meta-Analytic Evidence
| Outcome Measure | 6-Month Result | 12-Month Result | P-Value |
|---|---|---|---|
| Total WOMAC | MD = 7.44 (95% CI 1.45–13.42) | MD = 10.31 (95% CI 0.96–19.67) | P=0.01 / P=0.03 |
| WOMAC Pain | MD = 1.13 | MD = 1.03 | P=0.001 / P=0.04 |
| WOMAC Stiffness | MD = 0.49 | MD = 0.65 | P=0.01 / P=0.04 |
| WOMAC Function | MD = 3.36 | MD = 0.82 (ns) | P=0.006 / P=0.76 |
| 100-mm VAS Pain | MD = 19.39 | MD = 16.21 | P=0.0008 / P=0.0003 |
| Adverse Events (vs control) | No significant difference | — | P=0.21 (ns) |
| Serious Adverse Events (vs control) | No significant difference | — | P=0.69 (ns) |
The Cao et al. 2025 meta-analysis is the strongest current evidence summary. It pooled 8 RCTs of 502 knee osteoarthritis patients who had not received any surgical treatment. The intervention was intra-articular injection of MSCs without any other adjuvant therapy. Across the full pooled cohort, MSC-treated patients showed statistically significant improvement over control at both 6 and 12 months in total WOMAC, WOMAC subscales (pain, stiffness, function), and 100-mm VAS pain score.
Equally important is what the meta-analysis found about safety: adverse events did not differ significantly between MSC and control groups (P=0.21), and serious adverse events also did not differ (P=0.69). For a regenerative therapy in 2025, this is a meaningful signal. Combined with a 5-year follow-up by Kim et al. 2022 showing no treatment-related adverse events across 5 years post-injection, the safety profile of autologous ADSC therapy is at least as favorable as conventional intra-articular treatments.
Outcomes by Kellgren-Lawrence Grade — I, II, III, and IV
| KL Grade | Disease Stage | Symptom Relief | Best Evidence | Treatment Recommendation |
|---|---|---|---|---|
| I | Early — minor osteophytes, normal joint space | Excellent (long-term) | Cao 2025 (durability), Kim 2022 (5-year) | Ideal candidate — combine with weight management and exercise |
| II | Mild — definite osteophytes, possible joint space narrowing | Excellent | Cao 2025 pooled, Kim 2022 | Strong candidate — high long-term benefit |
| III | Moderate — multiple osteophytes, joint space narrowing, sclerosis | Strong (Phase III RCT) | Kim 2023 Phase III RCT (n=261, VAS 25.2 vs 15.5, P=.004) | Strongest RCT evidence — primary indication for treatment |
| IV | Severe — large osteophytes, bone-on-bone joint space loss, deformity | Modest — pain relief but no structural rebuild | Cao 2025 (subgroup), Kim 2022 (long-term) | Consider when TKA contraindicated or declined — TKA preferred for surgical candidates with deformity |
KL Grade I-II — Early Disease — Best Long-Term Outcomes
For early-stage KL I-II disease, stem cell therapy is ideally positioned. The cartilage is thinning but still functional, the joint structure is preserved, and the regenerative environment is most responsive. Patients in this range typically experience the largest long-term benefit. Combined with weight management and targeted exercise, KL I-II patients can often delay or entirely avoid surgical intervention.
KL Grade III — Moderate Disease — Strongest RCT Evidence
KL Grade III is the grade where stem cell therapy has the strongest Phase III randomized controlled trial evidence. A 2023 Phase III, multicenter, double-blind, placebo-controlled trial (NCT03990805) of 261 patients with KL Grade 3 symptomatic knee osteoarthritis, published in The American Journal of Sports Medicine (Kim, Lee, Lee et al. 2023), showed that a single intra-articular injection of autologous culture-expanded ADMSCs produced significantly greater 100-mm VAS pain reduction (25.2 vs 15.5, P=.004) and total WOMAC improvement (21.7 vs 14.3, P=.002) than placebo at the 6-month primary endpoint, with no serious treatment-related adverse events.
KL Grade IV (Bone-on-Bone) — When Stem Cells Help and When Surgery Is Better
At KL Grade IV, stem cells will not rebuild the joint. What they can offer is meaningful pain reduction and functional improvement — particularly valuable for patients who cannot undergo TKA because of age, comorbidities, anticoagulation requirements, or personal preference. For surgical candidates with severe deformity, TKA remains the better long-term choice. For non-surgical candidates, stem cell therapy is the most effective non-surgical pain-and-function intervention currently supported by 2025 meta-analytic data.
How Many Stem Cells Do You Need? Why 100 Million Is the Threshold
| Dose Tier | Cells per Knee | 6-Month WOMAC Effect | 12-Month WOMAC Effect | Clinical Interpretation |
|---|---|---|---|---|
| Low | 10–64 million | MD = 3.20 (P=0.16, ns) | MD = 4.84 (P=0.03) | Marginal — below threshold for durable signaling |
| High | ≥100 million (1×10⁸) | MD = 8.14 (P=0.002) | MD = 14.25 (P<0.0001) | Significantly better at both time points — operational standard |
| CGC standard | Guaranteed ≥100 million ADSCs per knee | Follows Cao high-dose tier | Follows Cao high-dose tier | Cell Grand Clinic’s Grand Stem Cell protocol |
Why dose matters biologically is straightforward: stem cells exert their effects through paracrine signaling — molecules released into the joint at concentrations proportional to cell number. Below a threshold dose, the signaling cascade is too weak to durably modulate the inflammatory and reparative environment. The Cao 2025 subgroup analysis quantified this for the first time in pooled data.
This is also why early Phase I dose-escalation work added important nuance. The 2016 Phase I trial published in Stem Cells Translational Medicine (Pers, Rackwitz, Ferreira et al. 2016) randomized 18 patients with severe knee osteoarthritis to three dose cohorts (2 million, 10 million, or 50 million autologous adipose-derived stem cells) and found that even low-dose patients experienced significant WOMAC improvement at 6 months, with no serious adverse events across all cohorts. The takeaway is not “more is always better at any dose” — it is “100 million is the threshold below which the 2025 meta-analytic data become marginal.” Cell Grand Clinic guarantees a minimum of 100 million quality-verified ADSCs per knee treatment.
Torn Meniscus Without Surgery: A Stem Cell Treatment Option Read ArticleADSC vs BMAC vs Donor Stock Cells — Why Adipose Outperforms for Knees
| Property | ADSC (Autologous, Cultured) | BMAC (Bone-Marrow, Autologous) | Donor Stock (Mexico / Cayman / Panama) |
|---|---|---|---|
| Tissue source | Your own fat (outpatient liposuction) | Your own bone marrow (iliac aspirate) | Umbilical cord / Wharton’s jelly (donor) |
| Cao 2025 6-month WOMAC subgroup | MD = 7.53 (P<0.00001) | MD = -6.30 (P=0.27, ns) | Not included (variable quality) |
| Immune rejection risk | None (your own cells) | None (your own cells) | Theoretical — varies by HLA matching and product |
| Transmissible infection risk | None | None | Donor-dependent screening required |
| Batch pooling | None — dedicated to one patient | None | Yes — produced for general use |
| Cell harvest | Local anesthesia, ~30 min outpatient | Local / spinal anesthesia, more invasive | No patient harvest |
| Cells per gram of tissue | High (~500× bone marrow yield) | Lower | N/A (frozen product) |
| Regulatory framework | Japan MHLW Type 2 certified (Cell Grand Clinic) | Varies by jurisdiction | No equivalent national framework |
Three cell-source decisions actually matter for knee osteoarthritis: tissue of origin (adipose vs bone marrow), donor status (autologous vs allogeneic), and product format (cultured individual batch vs pooled stock).
On tissue of origin, the 2025 Cao subgroup data favor adipose. ADSCs are easier to harvest (a brief outpatient liposuction versus a bone marrow aspirate), more abundant per gram of tissue, and yielded the statistically significant 6-month WOMAC effect that BM-MSCs did not in the pooled analysis. A 2024 randomized study published in Journal of Translational Medicine (Sun, Zhai, Han et al. 2024) added biological context: clinical outcomes of autologous AD-MSC therapy correlate with each patient’s own stem cell stemness and senescence markers — meaning younger, less senescent cells produce better results, which is exactly what passage-limited culture is designed to preserve.
On donor status, autologous (your own cells) is the dominant safety choice. There is no risk of immune rejection, no risk of transmissible infection from a donor, and the dose is dedicated to one patient. Phase I dose-escalation work confirmed safety across multiple dose tiers (Pers et al. 2016).
On product format, individual-batch culture is the dominant quality choice. Many overseas clinics use donor-derived stock cells (often from umbilical cord or Wharton’s jelly), which are pooled and produced for general use rather than for the individual patient — leading to variable viability, contamination risk, and dose inconsistency. The next section explains why Japan’s regulatory framework excludes this approach.
Why Autologous in Japan, Not Donor Stock from Mexico or Cayman
The contrast is structural, not promotional. Under Japan’s Act on the Safety of Regenerative Medicine, every clinic providing cell-based therapy must submit treatment plans to an MHLW-certified review committee, undergo facility audits of the Cell Processing Center (CPC), report adverse events under continuous surveillance, and maintain informed-consent and traceability records. There are three risk classifications:
- Type I (highest risk): pluripotent cells, gene-modified cells, and other high-risk modalities
- Type II (moderate-to-high risk): autologous and allogeneic cell therapies including ADSC for joint disease
- Type III (lower risk): minimally processed autologous cells
Only after MHLW review and approval can a clinic legally administer the treatment under continuing oversight. Cell Grand Clinic holds one of the broadest portfolios in Japan: 13 MHLW-notified plans (10 Type II plus 3 Type III). Knee osteoarthritis autologous ADSC treatment is one of these notified plans — not off-label, not unregulated, but a government-reviewed protocol with documented dose, indication, and ongoing safety reporting.
By contrast, donor stock cells from overseas clinics in Mexico, Panama, or the Cayman Islands operate outside any equivalent national framework. They use cells produced for general use, with pooling across donors, frozen logistics chains, and variable viability — precisely the conditions that Japan’s framework was designed to exclude.
Cell Grand Clinic — Grand Stem Cell, ABRM Physician, 3,000+ Cases
Grand Stem Cell — Four Quality Standards (Fresh / Pure / Young / Dose)
Cell Grand Clinic’s Grand Stem Cell protocol guarantees four specific standards on every knee treatment.
1. Fresh — Cultured Exclusively for You, No Batch Pooling. Every batch of cells is expanded from your own fat tissue over a seven-week culture process, with every batch dedicated to one patient only. No pooling across patients. No frozen storage of finished product. The cells are delivered fresh, peaking in biological activity at the time of administration.
2. Pure — ISCT-Standard FACS Verification (CD73/CD90/CD105 near-100%). Surface-marker testing follows the global standard of the International Society for Cell & Gene Therapy. Cells must express CD73, CD90, and CD105 at near-100% positivity, and must be negative for hematopoietic markers (CD45, CD34). Cells that do not meet these defining mesenchymal stem cell criteria are discarded, not delivered.
3. Young — Passage 3 Strict Limit Preserves Regenerative Capacity. Stem cells age with each passage (laboratory division cycle). Grand Stem Cells are strictly limited to Passage 3 or below — a practice biologically validated by Sun et al. 2024, which showed that clinical outcomes correlate with cellular stemness and senescence markers.
4. Dose — Guaranteed 100 Million+ Cells, 95%+ Viability. Viability is verified at greater than 95% immediately before administration, with the dose guaranteed at a minimum of 100 million cells per knee — the threshold confirmed by 2025 Cao meta-analytic dose-response data.
Every patient at Cell Grand Clinic receives a Certificate of Quality documenting that their Grand Stem Cells met all four standards before administration.
Cell Quality: The Key Factor That Impacts Stem Cell Therapy Outcomes Learn More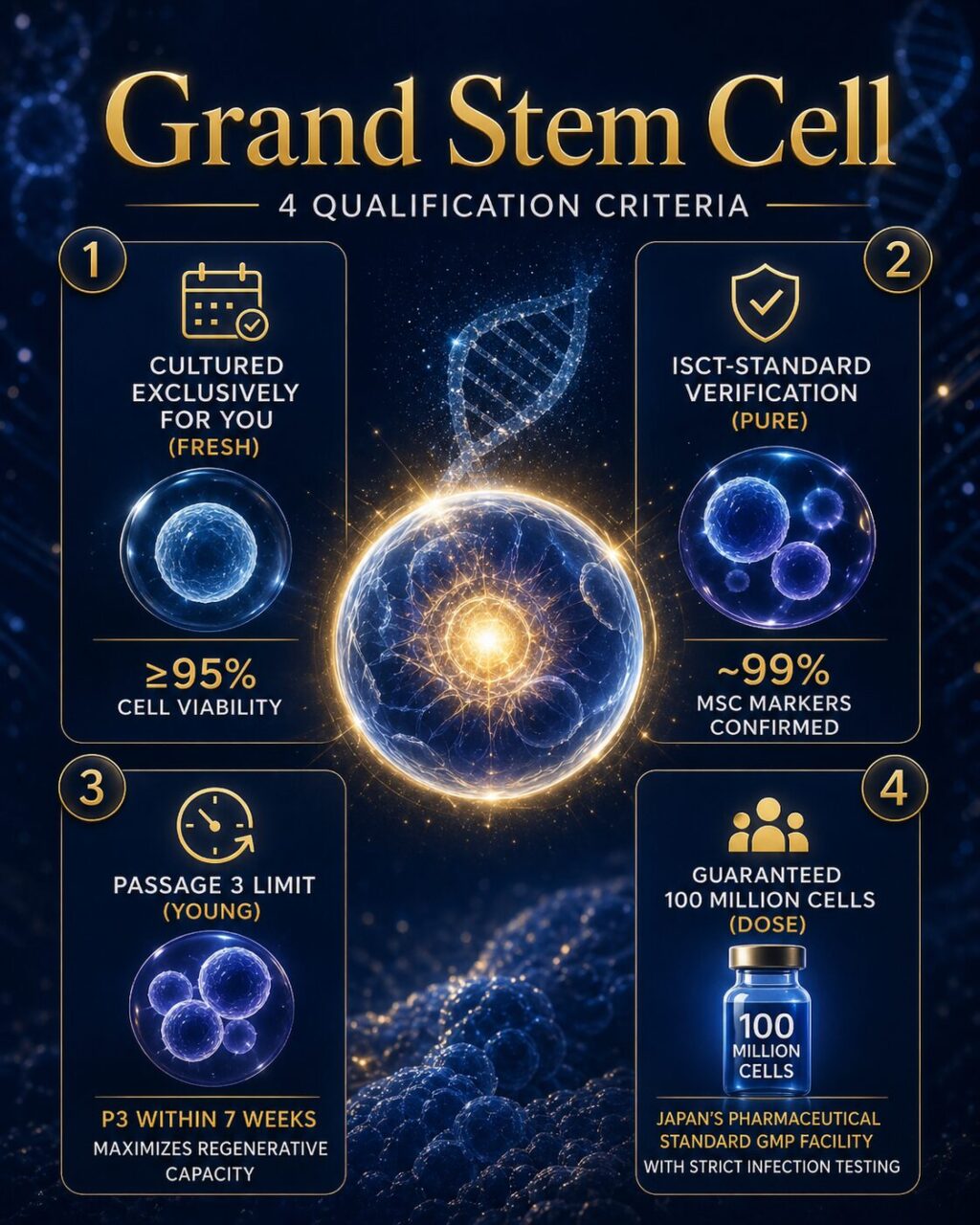
Dr. Yuichi Wakabayashi — ABRM, NIH-trained, 3,000+ Cases
Dr. Yuichi Wakabayashi, M.D., Ph.D., is American Board of Regenerative Medicine (ABRM) certified, NIH-trained, and has personally managed more than 3,000 stem cell cases across approximately 20 countries. He personally conducts every step of every patient’s treatment — consultation, fat harvest, supervision of cell culture, intra-articular injection, and 1/3/6-month follow-up. He has authored six peer-reviewed English-language publications. Cell Grand Clinic is featured in The Wall Street Journal (2025), is a Medical Excellence JAPAN member clinic, and is a 2026 Healthcare Business Review APAC Top Regenerative Medicine Solution in APAC awardee.
13 certified treatment plans (Type II and III licenses)
Cell Grand Clinic holds One of the broadest portfolios of any regenerative medicine clinic in Japan. Our knee OA treatment is not “experimental” or “off-label.” It is a government-regulated medical treatment.
Compare this to the situation in many other countries, where stem cell clinics operate with little regulatory oversight, using uncharacterized cell preparations with no quality control requirements.
Knee Stem Cell Treatment Process
- Online consultation — directly with Dr. Wakabayashi (English, no interpreter required) — review of X-rays, MRI, Kellgren-Lawrence grade assessment, and candidacy discussion.
- Visit 1 — Fat harvest under local anesthesia — a brief outpatient procedure, typically from the abdomen, of approximately 30 minutes. You walk out the same day.
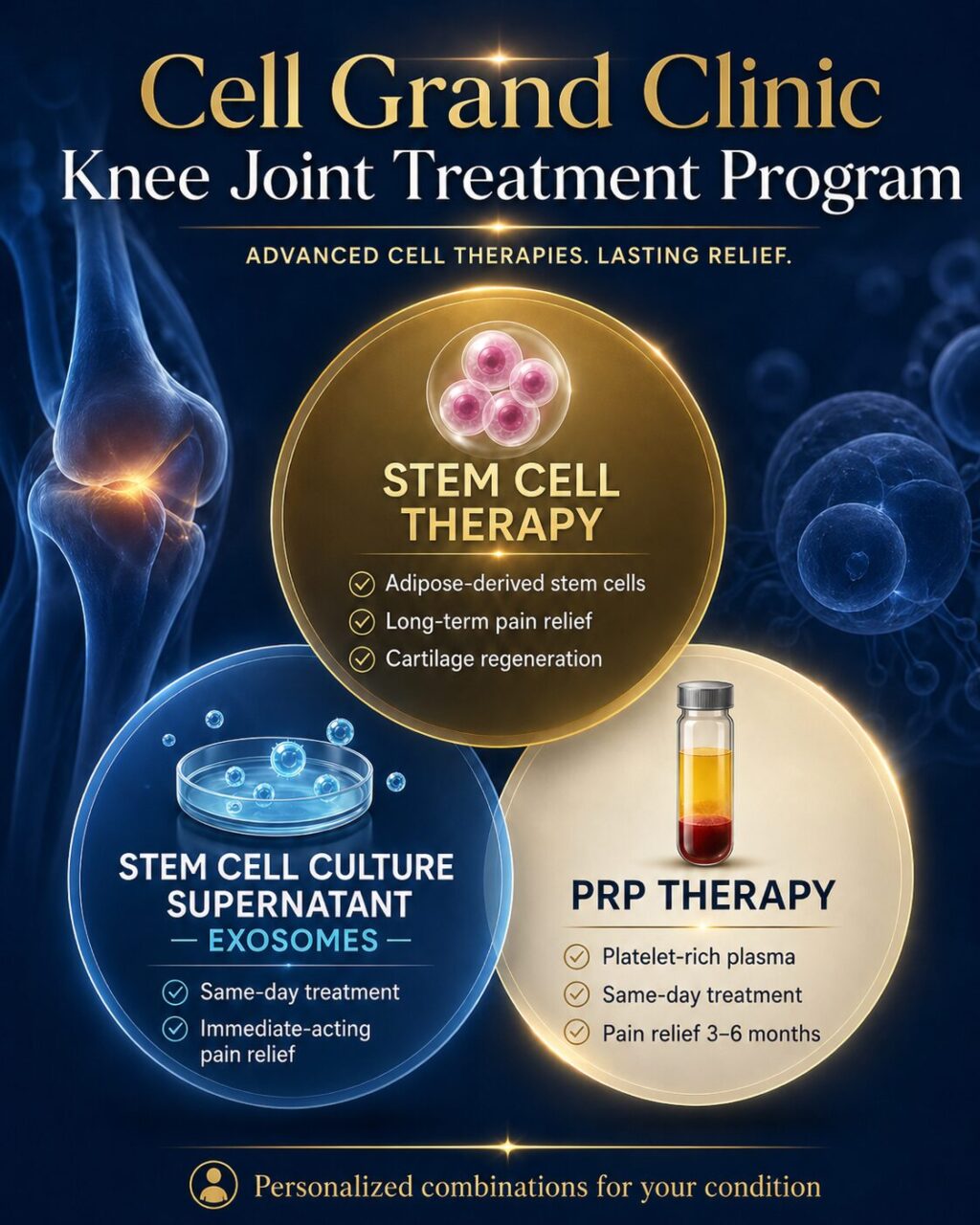
During Visit 1, your doctor may also administer Exosome Therapy or PRP (Platelet-Rich Plasma) injection directly into your knee. These treatments provide immediate anti-inflammatory and pain-relieving effects — helping you manage your current knee pain while your stem cells are being cultured over the next 7 weeks. Think of it as a “bridge treatment” that starts working right away, so you don’t have to endure unnecessary discomfort while waiting for your personalized stem cells to be ready. - Cell culture (7 weeks) — your fat-derived stem cells are expanded under MHLW-regulated Cell Processing Center conditions to a minimum of 100 million cells, strictly within Passage 3.
- Visit 2 — Intra-articular knee injection — same-day outpatient procedure under sterile conditions. You walk out of Cell Grand Clinic. No hospitalization required.
Most patients begin noticing reduced pain at 4-8 weeks after injection, with peak improvement at 3-6 months. You can also have remote follow-up at 1, 3, and 6 months — symptom tracking, range of motion, return-to-activity timeline.
Share your MRI/X-ray results with our medical team for preliminary assessment.
Minimally invasive fat harvest (~30 minutes) under local anesthesia. Return to your hotel immediately.
⚡ Don’t wait 7 weeks in pain
During Visit 1, your doctor may also administer Exosome Therapy or PRP (Platelet-Rich Plasma) injection directly into your knee. These treatments provide immediate anti-inflammatory and pain-relieving effects — helping you manage your current knee pain while your stem cells are being cultured over the next 7 weeks. Think of it as a “bridge treatment” that starts working right away, so you don’t have to endure unnecessary discomfort while waiting for your personalized stem cells to be ready.
Your cells are processed and expanded at our specialized CPC. Return home while we cultivate your cells to therapeutic levels — 100 million Grand Stem Cells.
✓ If you received Exosome/PRP in Visit 1, these continue working to relieve pain during this waiting period.
Return to Osaka for stem cell administration via direct intra-articular injection (~30 minutes including preparation).
Note: Repeat treatments may be recommended depending on disease severity.
Who Is a Candidate, and What Are the Pros and Cons?
This therapy is particularly effective for:
- Kellgren-Lawrence Grade II-III OA: Patients with moderate degeneration typically see the best outcomes
- Hyaluronic acid, steroid injections, or PRP no longer provide lasting relief
- Active individuals: Those who want to continue sports (golf, tennis, hiking) that may become impossible after joint replacement
- Surgery-averse patients: Those who cannot or prefer not to undergo general anesthesia and prolonged rehabilitation
- Patients seeking to delay surgery: Even in advanced cases, stem cell therapy can reduce pain and potentially postpone surgical intervention
Postpone the knee replacement — repair the cartilage first.
Stem cell therapy — from $19,800 USD per session
$19,800 USD includes:
- 100 million autologous ADSCs
- 7-week culture at MHLW-certified CPC · passage ≤3
- Quality certificate · 95%+ viability
- 1 / 3 / 6 month remote follow-up
Final pricing depends on your individual case:
- Combination protocols
- Multiple sessions
Have Dr. Wakabayashi review your case.
Share your medical history and current treatments. Dr. Wakabayashi reviews each international inquiry and responds with a written feasibility note, recommended protocol, and quote. Typical turnaround: 1–3 business days.
Frequently Asked Questions
Q1: Can stem cell therapy help knee osteoarthritis?
Yes. A 2025 meta-analysis of 8 RCTs and 502 patients published in Stem Cell Research & Therapy (Cao et al. 2025) confirmed that intra-articular MSC injection significantly improves WOMAC at 6 months (MD=7.44, P=0.01) and 12 months (MD=10.31, P=0.03), with adipose-derived cells outperforming bone-marrow cells. Outcomes vary by Kellgren-Lawrence grade and dose.
Q2: How much does stem cell therapy cost for knees in Japan?
At Cell Grand Clinic in Osaka, autologous ADSC stem cell therapy for knees starts from $20,000 USD per session, which includes 100 million autologous ADSCs, 7-week culture at an MHLW-certified Cell Processing Center, Certificate of Quality (95%+ viability), and 6/12-month remote follow-up. Final pricing depends on cell count, combination protocols, and number of sessions.
Q3: What is the success rate of stem cell therapy for osteoarthritis?
The 2025 Cao meta-analysis demonstrated statistically significant WOMAC improvement in the pooled MSC group at both 6 and 12 months, with high-dose adipose-derived protocols showing the largest effect sizes. A 2023 Phase III RCT in KL Grade 3 patients (Kim, Lee, Lee et al. 2023) showed VAS reduction of 25.2 versus 15.5 for placebo (P=.004) at 6 months. “Success” rates depend on KL grade, dose, and individual response — but the evidence base for symptomatic improvement at 6 and 12 months is strong.
Q4: How long do stem cell knee injections last?
Clinical evidence demonstrates sustained improvement at 12 months in the 2025 Cao meta-analysis, with 5-year durability documented for a single high-dose (1×10⁸ cells) autologous ADMSC injection in Kim et al. 2022 (Stem Cells Translational Medicine). Individual results vary based on KL grade, activity level, and overall health.
Q5: Is stem cell therapy effective for bone-on-bone (KL Grade IV) knees?
Stem cells cannot rebuild a fully collapsed joint surface. For KL Grade IV patients who cannot undergo TKA or who choose not to, stem cell therapy is the most effective non-surgical pain-and-function intervention available — based on Cao 2025 meta-analytic data — and can provide meaningful pain reduction and improved daily function for 1–2 years. For surgical candidates with severe deformity, TKA is the better long-term choice.
Q6: Where can I get stem cell therapy for knees?
Stem cell therapy for knees is available at clinics around the world, but quality and regulatory oversight vary dramatically. Cell Grand Clinic in Osaka, Japan delivers autologous ADSC therapy under MHLW Type 2 certification — Japan’s national regulatory framework for regenerative medicine — with up to 100 million quality-verified cells per knee and a Certificate of Quality for every patient.
Q7: Is ADSC better than BMAC for knees?
Yes, based on the 2025 Cao meta-analysis subgroup data: the ADSC subgroup showed significant 6-month WOMAC improvement (MD=7.53, P<0.00001), whereas the BM-MSC subgroup did not (MD=-6.30, P=0.27). ADSCs are also easier to harvest (outpatient liposuction versus bone marrow aspirate) and more abundant per gram of tissue.
Q8: Can foreign patients receive stem cell knee treatment in Japan?
Yes. Cell Grand Clinic treats international patients from approximately 20 countries. Dr. Wakabayashi conducts consultations in English directly (no interpreter required), and Cell Grand Clinic supports international patient logistics including pre-travel coordination, multilingual documentation, and remote 1/3/6-month follow-up.
Q9: Is there an age limit for knee stem cell therapy?
There is no fixed upper age limit. Cell Grand Clinic has successfully treated patients in their 80s. The 7-week culture protocol is especially important for older patients, because it allows expansion of cells with reduced proliferative capacity to the full therapeutic dose of 100 million cells, while remaining within the Passage 3 limit.
Conclusion: Restore Your Mobility — Naturally
For patients with moderate knee osteoarthritis seeking a non-surgical alternative, high-dose adipose-derived stem cell therapy offers a scientifically validated option. The 2025 meta-analysis confirmed that 100 million autologous MSCs injected into the knee significantly reduce pain and improve function for at least 12 months, with a safety profile comparable to placebo.
Cell Grand Clinic offers this scientifically validated, non-surgical solution for knee osteoarthritis — delivered under Japan's MHLW oversight with guaranteed quality through the Grand Stem Cell standard.
Reach us directly — WhatsApp and email inquiries are free of charge.
References
All citations are linked inline in the body of the article. Vancouver-style reference list:
- Cao M, Ou Z, Sheng R, et al. Efficacy and safety of mesenchymal stem cells in knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Stem Cell Res Ther. 2025;16(1):122. doi:10.1186/s13287-025-04252-2 (PMID 40055739)
- Kim KI, Lee MC, Lee JH, et al. Clinical Efficacy and Safety of the Intra-articular Injection of Autologous Adipose-Derived Mesenchymal Stem Cells for Knee Osteoarthritis: A Phase III, Randomized, Double-Blind, Placebo-Controlled Trial. Am J Sports Med. 2023;51(9):2243-2253. doi:10.1177/03635465231179223 (PMID 37345256)
- Kim KI, Lee WS, Kim JH, et al. Safety and Efficacy of the Intra-articular Injection of Mesenchymal Stem Cells for the Treatment of Osteoarthritic Knee: A 5-Year Follow-up Study. Stem Cells Transl Med. 2022;11(6):586-596. doi:10.1093/stcltm/szac024 (PMID 35567774)
- Song N, Scholtemeijer M, Shah K. Mesenchymal Stem Cell Immunomodulation: Mechanisms and Therapeutic Potential. Trends Pharmacol Sci. 2020;41(9):653-664. doi:10.1016/j.tips.2020.06.009 (PMID 32709406)
- Copp G, Robb KP, Viswanathan S. Culture-expanded mesenchymal stromal cell therapy: does it work in knee osteoarthritis? A pathway to clinical success. Cell Mol Immunol. 2023;20(6):626-650. doi:10.1038/s41423-023-01020-1 (PMID 37095295)
- Katz JN, Arant KR, Loeser RF. Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. JAMA. 2021;325(6):568-578. doi:10.1001/jama.2020.22171 (PMID 33560326)
- Pers YM, Rackwitz L, Ferreira R, et al. Adipose Mesenchymal Stromal Cell-Based Therapy for Severe Osteoarthritis of the Knee: A Phase I Dose-Escalation Trial. Stem Cells Transl Med. 2016;5(7):847-856. doi:10.5966/sctm.2015-0245 (PMID 27217345)
- Sun H, Zhai H, Han K, et al. Clinical outcomes of autologous adipose-derived mesenchymal stem cell combined with high tibial osteotomy for knee osteoarthritis are correlated with stem cell stemness and senescence. J Transl Med. 2024;22(1):1039. doi:10.1186/s12967-024-05814-3 (PMID 39558365)
Updated: 2026.05.28