Inquiries by Email
Inquiries by Email
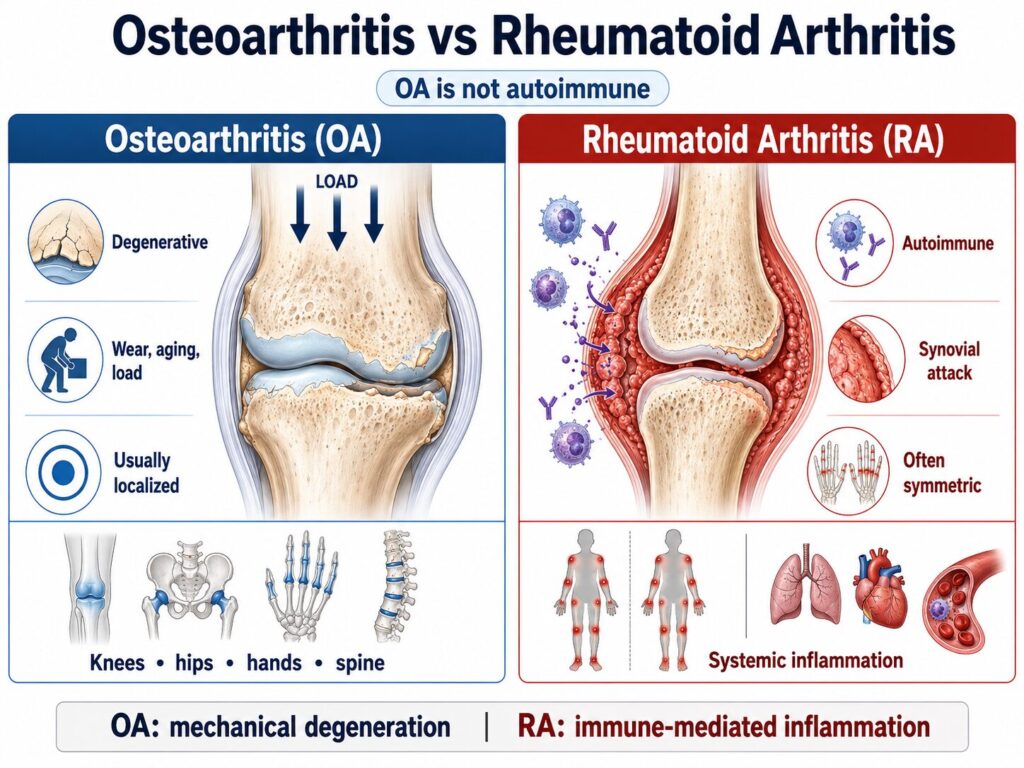
Osteoarthritis (OA) is a degenerative “wear-and-tear” disease of one or a few joints, while rheumatoid arthritis (RA) is a systemic autoimmune disease in which the immune system attacks the joint lining symmetrically across the body.
This guide compares their causes, symptoms, hand and X-ray patterns, diagnosis, and treatment — including where regenerative medicine fits for joint damage in Japan.
Cell Grand Clinic in Osaka, Japan uses your own adipose-derived stem cells (ADSCs), cultured for seven weeks to up to 200 million cells — never donor cells — delivered by intra-articular or IV administration.
MHLW-licensed. NIH-trained, ABRM-certified physician. 3,000+ treatments across ~20 countries.
- What’s the Difference Between Osteoarthritis and Rheumatoid Arthritis?
- Same Joint Pain, Two Very Different Diseases
- Is Osteoarthritis an Autoimmune Disease? (And Why RA Is)
- Symptoms Compared: How to Tell Them Apart
- In the Hands: Which Joints Each Affects
- Diagnosis: Blood Tests and X-ray Differences
- Can You Have Both? Can One Turn Into the Other?
- Which Is Worse — Osteoarthritis or Rheumatoid Arthritis?
- Treatment Options: Can Arthritis Be Reversed?
- Regenerative Medicine in Japan: Stem Cell Therapy for OA and RA
- Take the Next Step
- Frequently Asked Questions
- Take the Next Step
- References
What’s the Difference Between Osteoarthritis and Rheumatoid Arthritis?
The core difference between osteoarthritis and rheumatoid arthritis is the cause: osteoarthritis is mechanical joint damage from cartilage wearing down over time, while rheumatoid arthritis is an autoimmune disease in which the immune system mistakenly attacks the joints — meaning RA is systemic, often symmetric, and can affect the whole body.
That single distinction drives almost everything else — which joints are affected, how the pain behaves through the day, what shows up on blood tests and X-rays, and how each is treated. Here’s the practical breakdown most patients are actually looking for.
Same Joint Pain, Two Very Different Diseases
Both conditions cause joint pain and stiffness, but osteoarthritis affects roughly an order of magnitude more people than rheumatoid arthritis — and the two follow completely different paths, which is why an accurate diagnosis matters so much.
Why getting it right matters: rheumatoid arthritis can be slowed dramatically if it’s caught early and treated — so distinguishing it from ordinary wear-and-tear osteoarthritis is not just academic, it changes outcomes.
Is Osteoarthritis an Autoimmune Disease? (And Why RA Is)
No — osteoarthritis is not an autoimmune disease. It is a degenerative joint disease driven by mechanical wear, aging, and load on the cartilage. Rheumatoid arthritis, by contrast, is a systemic autoimmune disease: the immune system produces antibodies that attack the synovium (joint lining), causing body-wide inflammation.
This is the root reason the two behave so differently. Because RA is immune-driven, it tends to strike both sides of the body symmetrically and can also affect organs beyond the joints. Because OA is mechanical, it usually starts in the specific joints that have taken the most load over a lifetime — knees, hips, hands, and spine.
Symptoms Compared: How to Tell Them Apart
The fastest way to tell osteoarthritis from rheumatoid arthritis is the pattern of stiffness: OA stiffness is brief (under ~30 minutes) and worsens with use, while RA stiffness lasts longer (often over an hour each morning) and comes with systemic symptoms like fatigue and low-grade fever.
| Feature | Osteoarthritis (OA) | Rheumatoid Arthritis (RA) |
|---|---|---|
| Cause | Mechanical wear of cartilage | Autoimmune attack on joint lining |
| Morning stiffness | Brief (under ~30 min) | Prolonged (often over 1 hour) |
| Pattern | Often one-sided / asymmetric | Symmetric (both sides) |
| Pain with activity | Worse with use, better with rest | Better with movement, worse after rest |
| Whole-body symptoms | None | Fatigue, low fever, malaise |
| Onset age | Usually 50+ | Any age, often 30–60 |
If your stiffness eases within a few minutes of moving and stays in one or two joints, it points toward OA. If both hands are stiff for an hour every morning and you feel run-down, that pattern points toward RA and is worth an urgent rheumatology check.
In the Hands: Which Joints Each Affects
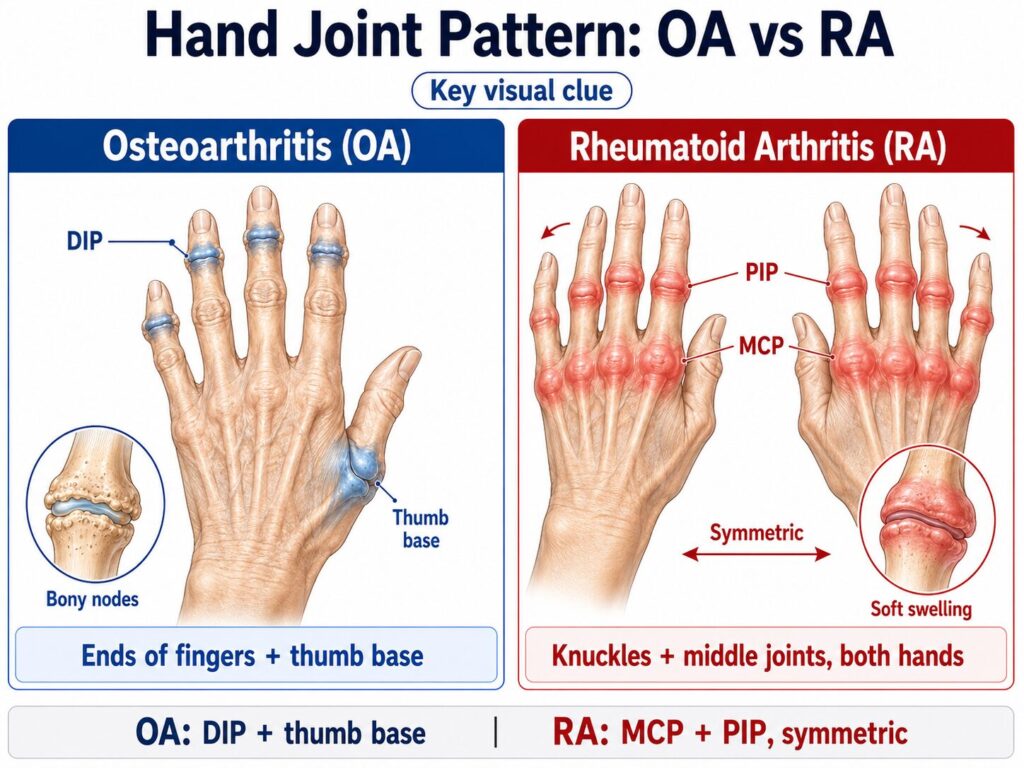
In the hands, osteoarthritis typically affects the joints closest to the fingertips (DIP) and the base of the thumb, while rheumatoid arthritis typically affects the knuckles (MCP) and middle finger joints (PIP) — symmetrically on both hands.
This hand pattern is one of the most reliable visual clues. OA tends to produce bony, knobby enlargements at the end finger joints (Heberden’s nodes). RA tends to produce soft, warm, swollen knuckles on both hands at once, and over time can cause the characteristic finger drift seen in advanced disease.
Diagnosis: Blood Tests and X-ray Differences
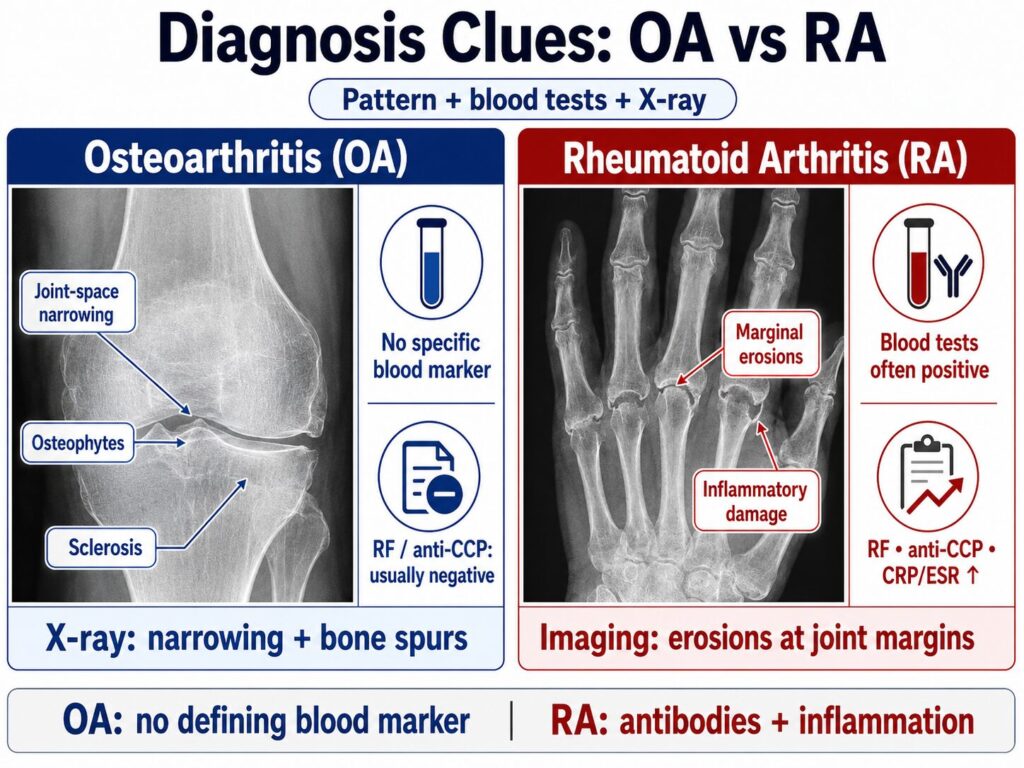
The decisive difference at diagnosis is that rheumatoid arthritis shows up in blood tests (rheumatoid factor, anti-CCP antibodies, elevated CRP/ESR) and produces joint erosions on imaging, while osteoarthritis has no defining blood marker and shows joint-space narrowing and bone spurs on X-ray.
Doctors combine three things: your symptom pattern, blood work, and imaging. In OA, blood tests are typically normal and X-rays show narrowed joint space, osteophytes (bone spurs), and hardened bone. In RA, antibodies and inflammatory markers are often elevated, and imaging shows inflammatory erosions at the joint margins.
Can You Have Both? Can One Turn Into the Other?
Yes, you can have both osteoarthritis and rheumatoid arthritis at the same time — this is common in older adults — but one does not turn into the other, because they have completely different mechanisms.
Osteoarthritis will not “become” rheumatoid arthritis: wear-and-tear damage cannot transform into an autoimmune disease. However, people with long-standing RA often develop secondary OA in joints that have already been damaged by inflammation, so both can genuinely coexist in the same person — and even in the same joint.
Which Is Worse — Osteoarthritis or Rheumatoid Arthritis?
Neither is simply “worse” — they’re serious in different ways: rheumatoid arthritis is potentially more dangerous because it is systemic and can damage organs and shorten life expectancy if untreated, while osteoarthritis is usually localized but is the leading cause of joint disability worldwide.
Untreated RA can affect the heart, lungs, eyes, and blood vessels, which is why early immune-modulating treatment is so important. OA rarely threatens other organs, but advanced OA can be profoundly disabling and is the most common reason for hip and knee replacement. Both deserve proper diagnosis and a treatment plan.
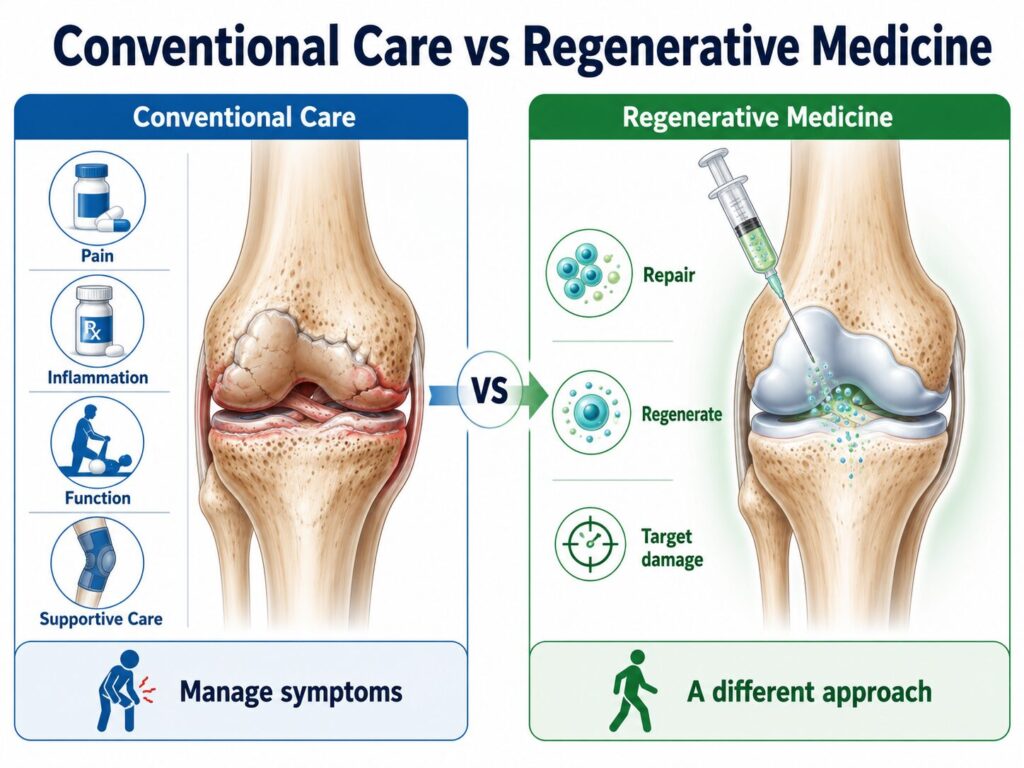
Treatment Options: Can Arthritis Be Reversed?
Conventional treatment cannot fully reverse either disease — OA care focuses on managing pain and preserving function, and RA care focuses on suppressing the immune attack with disease-modifying drugs — but regenerative medicine aims at the joint damage itself, which is a different approach.
For osteoarthritis, where the problem is worn cartilage, mesenchymal stem cell (MSC) therapy is being used to reduce pain and support cartilage, with the strongest evidence in the knee. For rheumatoid arthritis, the rationale is different: stem cells have natural immunomodulatory properties, and early-stage trials are studying whether they can calm the autoimmune process — this evidence is still developing, and stem cells are not a replacement for RA medication.
Regenerative Medicine in Japan: Stem Cell Therapy for OA and RA
In Japan, stem cell therapy for arthritis uses a patient’s own adipose-derived stem cells (ADSCs) under MHLW oversight, with the clearest results in osteoarthritis of the knee and an emerging, still-investigated role in rheumatoid arthritis.
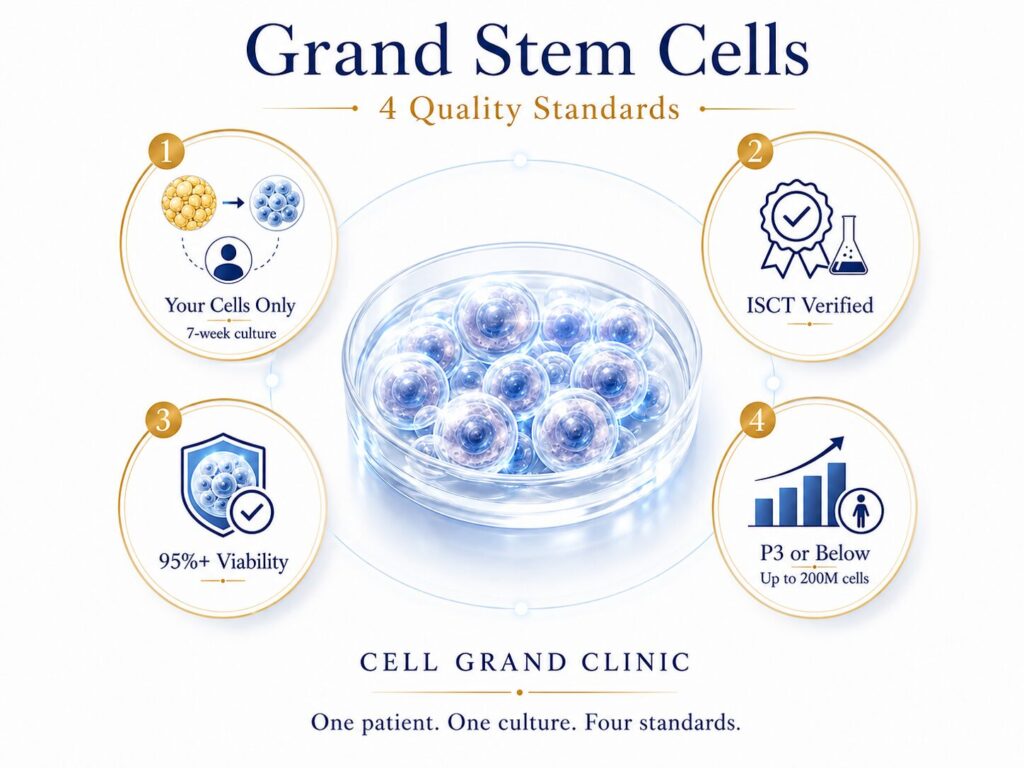
At Cell Grand Clinic, every treatment uses Grand Stem Cells — cultured exclusively for one patient, never pooled or off-the-shelf. Four standards define them: cells are cultured exclusively for you from your own fat tissue over seven weeks; each batch undergoes ISCT-standard verification to confirm genuine mesenchymal stem cells; only cells with 95%+ viability are administered; and culture is strictly limited to passage 3 or below to preserve youth and potency at up to 200 million cells. Every patient receives a Certificate of Quality documenting all four.
The table below compares the regulatory and quality framework patients weigh when choosing where to be treated.
| Factor | Japan (MHLW) | Many overseas clinics |
|---|---|---|
| Government oversight | MHLW-notified plan ✓ | Varies by country |
| Cell source | Your own (autologous) ✓ | Often donor / pooled |
| Quality standard | ISCT-verified, passage ≤3 ✓ | Varies by clinic |
| Physician | NIH-trained, ABRM ✓ | Varies |
Comparison is based on general regulatory frameworks; individual clinics vary. Japan’s regenerative-medicine law provides government-level oversight for cultured autologous cell treatments.
Take the Next Step
You don’t have to live with joint pain indefinitely — and you don’t need to commit to anything to find out whether stem cell therapy could help your specific case.
When you reach out, here’s what happens within 24 hours:
- Your case is reviewed personally by Dr. Yuichi Wakabayashi, ABRM — not a sales coordinator
- You receive a case feasibility assessment based on your medical history
- You get a clear price estimate and treatment timeline tailored to your situation
- You decide whether to proceed — with no obligation and no pressure
Most international patients use this consultation simply to understand their options. About a third decide to proceed; the rest leave with a clearer picture of where they stand.
Available in English, Japanese, and Mandarin Chinese · Response under 24 hours, Japan time
Frequently Asked Questions
Is osteoarthritis the same as rheumatoid arthritis?
No. Osteoarthritis is a degenerative “wear-and-tear” disease of specific joints; rheumatoid arthritis is a systemic autoimmune disease that attacks the joints symmetrically and can affect the whole body.
Which is worse, osteoarthritis or rheumatoid arthritis?
They’re serious differently. RA can be more dangerous because it’s systemic and can harm organs if untreated; OA is usually localized but is the leading cause of joint disability and joint replacement.
Can you have both osteoarthritis and rheumatoid arthritis?
Yes. Both can occur in the same person — and even the same joint — especially in older adults, because RA-damaged joints often develop secondary OA.
Can osteoarthritis turn into rheumatoid arthritis?
No. They have different mechanisms, so OA cannot become RA. A person can develop both separately, but one does not convert into the other.
Can arthritis be reversed?
Conventional treatment manages arthritis rather than reversing it. Regenerative medicine targets the joint damage directly; for knee osteoarthritis, stem cell therapy has shown significant pain and function improvement in trials, while the evidence in rheumatoid arthritis is still developing.
How do doctors tell osteoarthritis and rheumatoid arthritis apart?
By combining symptom pattern, blood tests (rheumatoid factor, anti-CCP, CRP/ESR), and imaging. RA shows antibodies and erosions; OA shows normal blood work with joint-space narrowing and bone spurs.
Stem Cell Therapy Pricing — From $19,800 USD per session
$19,800 USD includes:
- 100 million autologous ADSCs
- 7-week culture at MHLW-certified CPC
- Quality certificate · 98%+ viability
- 6 + 12 month remote follow-up
Final pricing depends on your individual case:
- Higher cell counts (200 million+)
- Combination protocols
- Multiple sessions
Take the Next Step
You don’t have to live with joint pain indefinitely — and you don’t need to commit to anything to find out whether stem cell therapy could help your specific case.
When you reach out, here’s what happens within 24 hours:
- Your case is reviewed personally by Dr. Yuichi Wakabayashi, ABRM — not a sales coordinator
- You receive a case feasibility assessment based on your medical history
- You get a clear price estimate and treatment timeline tailored to your situation
- You decide whether to proceed — with no obligation and no pressure
Most international patients use this consultation simply to understand their options. About a third decide to proceed; the rest leave with a clearer picture of where they stand.
Available in English, Japanese, and Mandarin Chinese · Response under 24 hours, Japan time
References
According to PubMed:
- Di Matteo A, Bathon JM, Emery P. Rheumatoid arthritis. Lancet. 2023;402(10416):2019-2033. https://doi.org/10.1016/S0140-6736(23)01525-8
- Finckh A, Gilbert B, Hodkinson B, et al. Global epidemiology of rheumatoid arthritis. Nat Rev Rheumatol. 2022;18(10):591-602. https://doi.org/10.1038/s41584-022-00827-y
- Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568-578. https://doi.org/10.1001/jama.2020.22171
- Cao M, Ou Z, Sheng R, et al. Efficacy of mesenchymal stem cells for knee osteoarthritis: a meta-analysis. Stem Cell Res Ther. 2025;16(1):122. https://doi.org/10.1186/s13287-025-04252-2
- Kim KI, Lee MC, Lee JH, et al. Intra-articular injection of autologous adipose-derived stem cells for knee osteoarthritis: a Phase III trial. Am J Sports Med. 2023;51(9):2243-2253. https://doi.org/10.1177/03635465231179223
- Kim KI, Lee WS, Kim JH, et al. Five-year follow-up of autologous adipose-derived stem cell injection for knee osteoarthritis. Stem Cells Transl Med. 2022;11(6):586-596. https://doi.org/10.1093/stcltm/szac024
- Zeng L, Liu C, Wu Y, et al. Efficacy and safety of MSC transplantation in autoimmune and rheumatic immune diseases: a systematic review and meta-analysis of RCTs. Stem Cell Res Ther. 2025;16(1):65. https://doi.org/10.1186/s13287-025-04184-x
- Mesa LE, López JG, López Quiceno L, et al. Safety and efficacy of mesenchymal stem cell therapy in rheumatoid arthritis: a systematic review and meta-analysis. PLoS One. 2023;18(7):e0284828. https://doi.org/10.1371/journal.pone.0284828
- Song N, Scholtemeijer M, Shah K. Mesenchymal stem cell immunomodulation: mechanisms and therapeutic potential. Trends Pharmacol Sci. 2020;41(9):653-664. https://doi.org/10.1016/j.tips.2020.06.009
Updated: 2026.06.08