Inquiries by Email
Inquiries by Email
Drug-free hair loss treatment in Japan uses adipose-derived mesenchymal stem cells (autologous ADSC) to reactivate dormant follicles — a non-surgical alternative to finasteride, minoxidil, and hair transplant.
Finasteride blocks DHT, minoxidil maintains the growth phase, and hair transplant relocates existing follicles. Stem cells regenerate the dermal papilla itself — under MHLW oversight in Japan.
At Cell Grand Clinic in Osaka, Japan, stem cells from your own fat are expanded over 7 weeks — up to 200 million microinjected into the scalp. No daily pill, no scalpel, no donor.
MHLW Type 2 certified. NIH-trained physician. 3,000+ cases.
- Why People Look Beyond Finasteride and Minoxidil
- What Is Stem Cell Therapy for Hair Loss?
- What Are AGA and FAGA? Why Your Follicles Aren’t Dead
- How Stem Cell Therapy Reverses Hair Loss: The Science, Made Simple
- Non-Surgical Hair Restoration: What Are Your Options?
- Does Stem Cell Work for Hair Loss? Clinical Evidence
- Where Stem Cell Therapy Fits Among Drug-Free Options
- Your Treatment at Cell Grand Clinic: Step by Step
- What to Expect: Your Results Timeline
- Who Is the Ideal Candidate?
- Hair regeneration without lifelong medication.
- Frequently Asked Questions
- Closing: Why Now?
- References
Why People Look Beyond Finasteride and Minoxidil
Finasteride and minoxidil have been the standard pharmaceutical options for androgenetic alopecia (AGA) since the 1990s. They work — partially — but their limitations drive an estimated 30–40% of users to discontinue treatment within two years.
Finasteride (Propecia, Proscar): Blocks the conversion of testosterone to DHT, the hormone that miniaturizes follicles. Effective for many men, but documented side effects include sexual dysfunction (3–15% of users), reduced libido, and mood changes. A subset of patients report “post-finasteride syndrome” — persistent symptoms after stopping the drug. Off-label use in women is limited because of teratogenic risk; use during pregnancy is contraindicated.
Minoxidil (Rogaine): A topical vasodilator that prolongs the anagen (growth) phase. Requires twice-daily application indefinitely; results plateau when treatment stops. Response rates in clinical trials hover around 40–60%, with the most pronounced effect in men under 40 with recent-onset thinning.
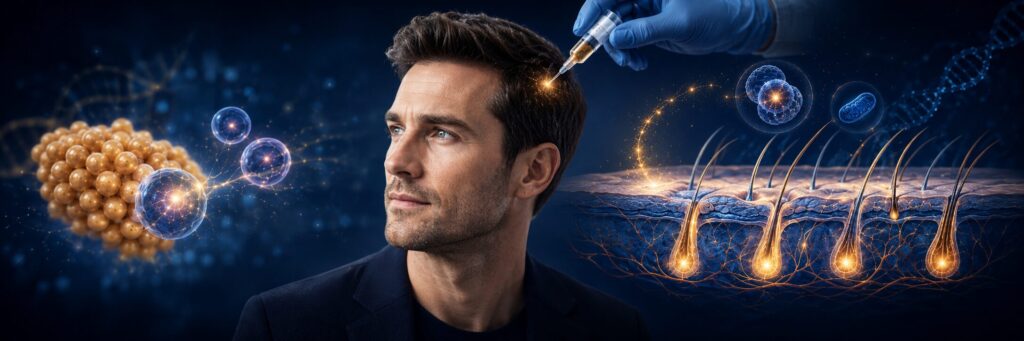
Both treatments manage the disease process. Neither regenerates lost follicles or rebuilds the dermal papilla — the cellular structure that actually controls hair production. For patients who have stopped responding to drugs, experienced side effects, or want a treatment that addresses the biological cause rather than the symptom, regenerative options have become the natural next step.
Stem cell therapy belongs to a newer category: biological regeneration. Instead of blocking a hormone or stimulating circulation, it restores the microenvironment that dormant follicles need to grow again. The next section explains how this works in the scalp.
What Is Stem Cell Therapy for Hair Loss?
Stem cell hair restoration uses a patient’s own fat-derived stem cells to reverse hair loss by rebuilding blood supply, reactivating dormant follicles, and repairing damaged structures. Learn more about how stem cell quality affects outcomes in our research library.
The Biology Behind Hair Loss
In male pattern hair loss (AGA), hair follicles shrink from thick, rooted structures to thin, superficial ones. In female pattern hair loss (FPHL), women lose density across the scalp. But here’s the critical discovery: the follicle stem cells aren’t dead.
Garza and colleagues at the University of Pennsylvania, published in the Journal of Clinical Investigation (2011), proved that even in bald scalps, follicle stem cells persist — the problem is in stem-to-progenitor conversion, not cell death. Matsumura et al. later showed in Science (2016) that COL17A1 deterioration causes stem cells to emigrate from follicles over time. This matters because dormant cells can be reactivated. Dead cells cannot.
What Are AGA and FAGA? Why Your Follicles Aren’t Dead
Androgenetic Alopecia (AGA) is genetically driven hair loss—commonly known as male pattern baldness. In women, it’s called Female Androgenetic Alopecia (FAGA) or female pattern hair loss. By age 50, roughly half of all men and nearly 40% of women experience noticeable thinning, and many notice changes as early as their late 20s.
Here’s what’s happening beneath the surface: dihydrotestosterone (DHT) binds to receptors in genetically susceptible follicles and gradually shrinks them. The growth phase (anagen) shortens cycle by cycle until each hair becomes too thin and short to see.
But here’s the critical point: in most AGA and FAGA cases, the follicle stem cells are still alive. They’re miniaturized and dormant—not dead. Research published in the Journal of Clinical Investigation confirmed that even in bald scalps, follicle stem cells remain present in the bulge region (Garza et al., 2011). They simply lack the right signals to reactivate.
This is precisely why stem cell therapy works—and why drugs that only block DHT can never fully reverse the damage.
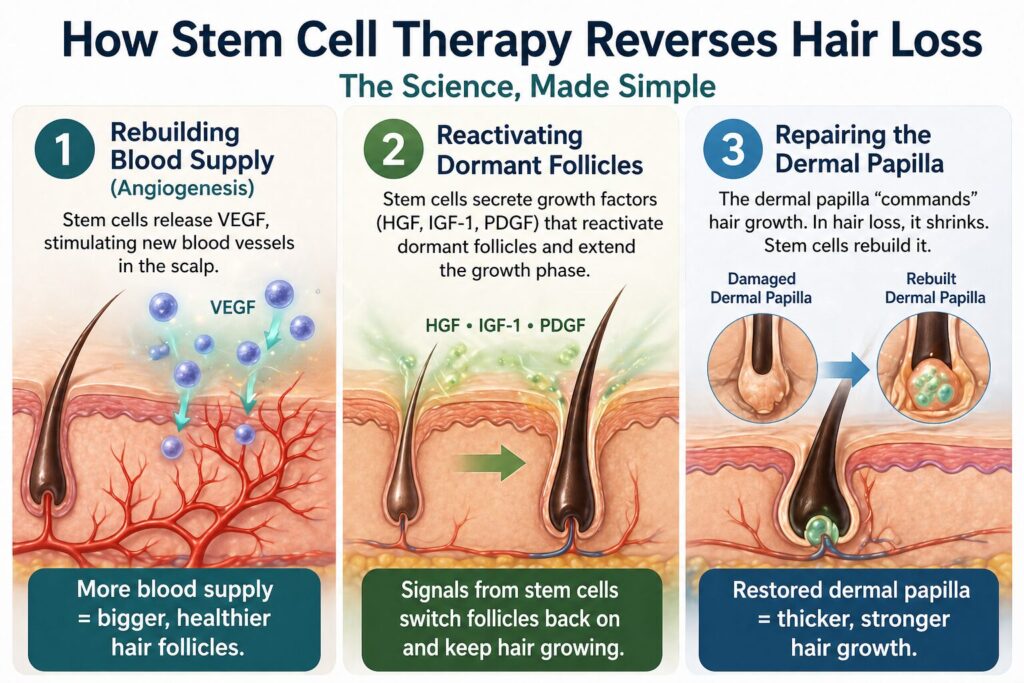
How Stem Cell Therapy Reverses Hair Loss: The Science, Made Simple
Stem cell therapy rebuilds the biological infrastructure damaged by hair loss. Three mechanisms:
Rebuilding Blood Supply (Angiogenesis)
Adipose-derived stem cells secrete VEGF (vascular endothelial growth factor), stimulating new blood vessels in the scalp. Yano et al. demonstrated in the Journal of Clinical Investigation (2001) that VEGF-mediated angiogenesis directly controls follicle size and hair growth — in plain terms, more blood supply means bigger, healthier follicles.
Reactivating Dormant Follicles
Stem cells secrete growth factors (HGF, IGF-1, PDGF) that reactivate dormant follicles and extend the growth phase. The signals stem cells produce drive recovery.
Repairing the Dermal Papilla
The dermal papilla “commands” hair growth. In hair loss, it shrinks. Stem cells rebuild it. Thicker dermal papillas = thicker hair growth.
Non-Surgical Hair Restoration: What Are Your Options?
For patients who reject hair transplant — typically because of cost ($15,000–$50,000), recovery time, or the risk of an unnatural-looking hairline — several non-surgical options have emerged. Not all are equally evidence-backed.
| Option | What It Does | Strength of Evidence | Typical Limitation |
|---|---|---|---|
| Low-Level Laser Therapy (LLLT) | Photobiomodulation of follicles via red light | Moderate; FDA-cleared for some devices | Requires daily 20–30 min sessions for months |
| Microneedling | Mechanical injury to trigger growth factor release | Limited as monotherapy; used as adjunct | Modest gains, often combined with PRP or minoxidil |
| Platelet-Rich Plasma (PRP) | Injects concentrated growth factors from your blood | Moderate; multiple RCTs show density gains | 3–6 sessions, results fade within 12 months |
| Exosome Therapy | Cell-derived signaling vesicles applied topically or injected | Emerging; mostly observational data | Quality varies widely between providers |
| Autologous Stem Cell (ADSC) | Live regenerative cells that rebuild the follicular environment | Strong; published RCTs with sustained 12+ month results | Available only at licensed regenerative clinics |
| Hair Transplant (FUE/FUT) | Surgical relocation of donor follicles | Strong; mechanical solution | Surgical risks; cannot regenerate lost follicles, only redistribute them |
Where stem cell therapy stands apart: PRP and exosome treatments deliver growth factors. Stem cells deliver the cells that produce those growth factors continuously, plus the cellular machinery to rebuild blood vessels and dermal papilla structure. This is why autologous ADSC results last 12+ months in clinical follow-up, while PRP typically requires quarterly maintenance.
For patients evaluating alternatives to hair transplant specifically: stem cell therapy is the only non-surgical option with published evidence for regenerating thinning follicles (rather than only relocating existing ones). It cannot, however, restore follicles that have been completely gone for years — early intervention matters.
Note that ‘stem cell hair transplant’ is sometimes used colloquially to refer to stem cell-enhanced FUE protocols, but autologous ADSC therapy is fundamentally non-surgical — no follicular unit extraction, no donor area, no incision.
Does Stem Cell Work for Hair Loss? Clinical Evidence
A 2024 systematic review of 12 RCTs and a 2023 meta-analysis of stem cell-derived conditioned media — together with multiple individual RCTs — show statistically significant increases in hair count and density across stem cell-based approaches. No serious adverse events have been reported across the included trials, though minor injection-site reactions are common.
It’s important to note: the published trials use multiple cell sources (adipose, hair follicle, bone marrow, umbilical cord blood, and dental pulp) and different preparations (cultured cells, stromal vascular fraction, conditioned media, secretome). Outcomes and mechanisms can differ across these.
Evidence Table: What Clinical Trials Show
Clinical trials demonstrate consistent improvements in hair density and count across multiple patient populations. The table below reflects published, peer-reviewed evidence from randomized controlled trials and systematic reviews.
| Study | Year | Design | Patients (n) | Cell Type | Key Finding | Follow-up |
|---|---|---|---|---|---|---|
| Gasteratos et al. PRS Glob Open | 2024 | Systematic review (12 RCTs) | 514 | Mixed sources: adipose, hair follicle, bone marrow, umbilical cord, dental pulp | Stem cell-derived therapies improved hair regeneration; no serious adverse events | 2013–2023 |
| Chien et al. JPRAS | 2023 | SR & Meta-analysis | 221 | Mostly ADSC-derived conditioned media | MD hair density +14.93/cm² (p<0.0001); MD thickness +18.67 μm | Varied |
| Tak et al. Stem Cells Transl Med | 2020 | RCT, double-blind | 38 | ADSC constituent extract (topical, acellular) | Hair count +28.1% vs +7.1% control (p<0.05); diameter +14.2% vs +6.3% control | 16 wk |
| Moneib et al. Int J Trichology | 2025 | Controlled trial (3 severity groups) | 33 women | Cultured autologous ADSC, intrascalp injection (★ same cell type as our protocol) | Density, thickness, follicular units improved; ↑follistatin, ↓DKK-1 | 12 & 24 wk |
| Gentile Int J Mol Sci | 2019 | Controlled, half-head | 33 | HD-AFSC micrograft from scalp biopsy (mechanical fragmentation, uncultured) | 33%±7.5% density at 23 wk (declined to 27%±3.5% at 44 wk); follicle density 0.46→1.4/mm² at 11 mo | 23–44 wk |
| Shin et al. Int J Dermatol | 2015 | Retrospective | 27 | ADSC conditioned media (acellular) | Hair density 105.4→122.7/cm² (16.4%); thickness 57.5→64.0 μm | 12 wk |
| Legiawati et al. Arch Dermatol Res | 2025 | Comparative (3 groups) | 60 | ADSC secretome (acellular) | Combination of ADSC-CM + minoxidil produced the best improvement | 12 wk |
All studies used human subjects. Full references with DOI links are provided at the end of this article.
What These Studies Show — and What They Don’t
The most relevant study for our protocol is Moneib et al. 2025 (Int J Trichology, DOI). This is one of the few published trials using cultured autologous adipose-derived stem cells injected directly into the scalp — the same cell category used at Cell Grand Clinic. In 33 women with FPHL, hair density, thickness, and follicular unit count improved at 12 and 24 weeks, with measurable changes in hair cycle markers (↑follistatin, ↓DKK-1).
The largest review is Gasteratos et al. 2024 (PRS Glob Open, DOI), covering 12 RCTs and 514 patients across multiple cell sources (adipose, hair follicle, bone marrow, umbilical cord, dental pulp). The review confirms safety and efficacy signals across cell types, while noting that direct head-to-head comparisons between sources are limited.
The most quantitative analysis is Chien et al. 2023 (J Plast Reconstr Aesthet Surg, DOI), a meta-analysis specifically of stem cell-derived conditioned media (mostly ADSC-derived). Across 8 trials (n=221), the pooled mean difference in hair density was +14.93/cm² (95% CI: 10.20–19.67, p<0.0001). The RCT subgroup analysis showed +9.23/cm² (CI: 1.79–16.68).
Where Stem Cell Therapy Fits Among Drug-Free Options
Patients seeking drug-free hair loss treatment usually rank options by three criteria: evidence quality, durability of results, and regulatory standing of the provider.
Evidence quality. Among drug-free options, autologous stem cell therapy has the strongest published RCT data for AGA and FAGA — including the +33% hair density figure cited above, drawn from 24-week controlled trials. LLLT, PRP, and microneedling all have evidence, but typically in shorter follow-up windows or smaller sample sizes.
Durability. Drug-free does not mean “no maintenance” by default. PRP and exosome treatments commonly require quarterly sessions to sustain results. A single autologous ADSC course produces gains visible at 12 months in follow-up cohorts, with optional booster therapy after 18–24 months for patients with progressive AGA.
Regulatory standing. This is where treatment quality varies most internationally. Stem cell therapies offered as “regenerative medicine” in many countries operate without specific oversight. Japan is one of the few jurisdictions with a dedicated regulatory framework for regenerative medicine, established by the Ministry of Health, Labour and Welfare (MHLW) under the Act on the Safety of Regenerative Medicine. Cell Grand Clinic operates under 13 MHLW-approved treatment plans (10 Class II + 3 Class III) — among the highest in Osaka — meaning every cell processing step is government-overseen, every adverse event is reportable, and every treatment plan is subject to ethics committee review.
For international patients specifically, this translates into three practical advantages over treatment in less-regulated markets:
- Cell quality is standardized. ISCT-criteria flow cytometry confirms CD73/CD90/CD105 expression at near-100%; viability is validated above 95% before infusion; no batch-pooling between patients.
- Provider accountability is enforced. Treatments are physician-led end-to-end rather than delegated to technicians.
- Documentation is portable. Treatment records meet international regulatory standards, useful if you need follow-up care in your home country.
Stem cell therapy is not the only drug-free option for hair loss, but it is the option with the strongest evidence, the longest-lasting results, and — at MHLW-licensed clinics in Japan — the most rigorous quality control available globally.
- ✓ Diplomate, American Board of Regenerative Medicine (ABRM) — one of the few in Asia
- ✓ Former NIH research fellow; first-author on world’s first-in-human PDE4B PET tracer (with Pfizer)
- ✓ 3,000+ stem cell procedures across 20+ countries of patient origin
- ✓ Featured in The Wall Street Journal; member of Medical Excellence JAPAN (MEJ)
- ✓ All consultations conducted directly in English — no interpreter required
Your Treatment at Cell Grand Clinic: Step by Step
Our protocol is designed specifically for international patients. The entire process requires just two visits to Osaka, approximately 7–8 weeks apart (the time required for safe cell cultivation).
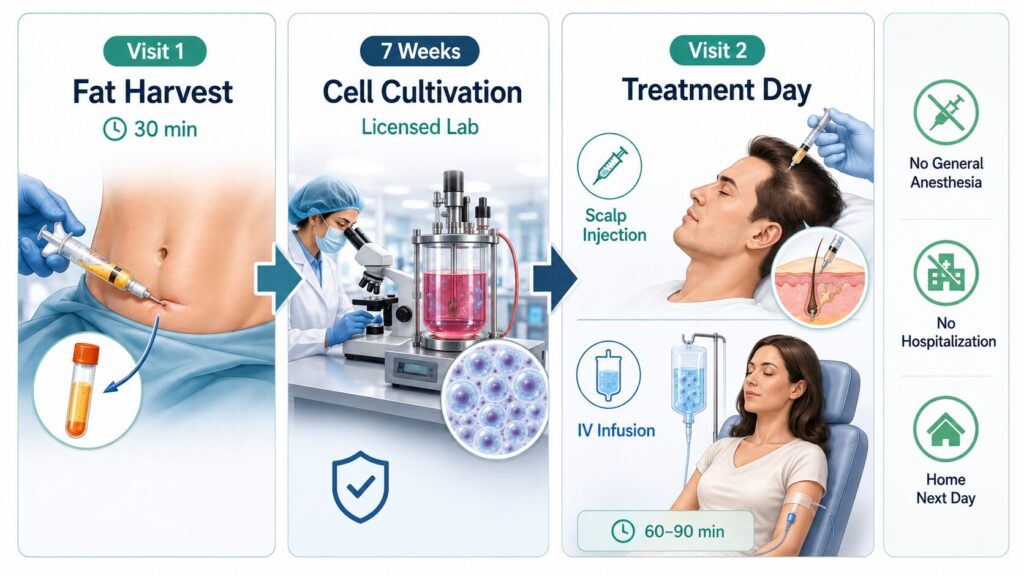
Visit 1: Fat Harvest (30 Minutes)
Under local anesthesia, approximately 10ml of fat is extracted from your abdomen through a small incision. You can resume normal activities the same day.
Note: Cell Grand Clinic can provide stem cell-derived conditioned media on the same day to enhance hair regeneration
Weeks 1–7: Cell Cultivation in Our Licensed Laboratory
Your tissue is transported to our government-certified Cell Processing Center, where stem cells are isolated and cultured to reach 100 to 200 million cells with over 95% viability. Every batch is tested for sterility, viability, and potency before treatment.
Visit 2: Dual-Delivery Treatment Day
Direct Scalp Injection delivers stem cells precisely into the dermal papilla layer—exactly where follicle regeneration needs to happen. This targeted approach maximizes concentration where it matters most. IV Infusion (optional but recommended) delivers stem cells systemically, supporting vascular health and overall regeneration. Many patients combine scalp treatment with broader anti-aging benefits. Total treatment time: approximately 60–90 minutes. No general anesthesia. No hospitalization. Fly home the next day.
Exosome Therapy: Same-Day, Cell-Free Regeneration Learn More Reverse Aging: How Stem Cell IV Therapy Actually Works Learn How Stem Cell Therapy in Japan: Plans, Pricing & What to Expect Read GuideReach us directly — WhatsApp and email inquiries are free of charge.
What to Expect: Your Results Timeline
| Timeframe | What to Expect |
|---|---|
| Weeks 1–4 | Reduced shedding; early signs of follicle reactivation beginning at the cellular level. |
| Weeks 4–12 | New fine hairs (vellus) emerging; existing hairs may begin to feel thicker. |
| Months 3–6 | Visible improvement in density and thickness. Clinical trials show statistically significant results by week 8–16. |
| Months 6–12 | Peak results—fuller, thicker, stronger hair. Many patients report the improvement continues beyond the 6-month mark. |
| 12+ Months | Sustained results. Annual maintenance treatment recommended for long-term optimization. |
Individual results vary depending on the degree of hair loss, overall health, and genetics. Patients with earlier-stage AGA/FAGA typically see the most dramatic improvements—another reason not to delay.
Who Is the Ideal Candidate?
Stem cell hair restoration works best for certain patients. Here’s how to assess your candidacy.
Norwood-Hamilton I–V or Ludwig I–II classification
Rather than decades-long stable baldness
Even if miniaturized; these can be reactivated
Stem cell therapy is gradual and natural-looking
Logistics can be coordinated with the clinic
These must be managed before treatment
Very few follicles remain to reactivate
Scarred follicles cannot regenerate; new follicles cannot grow in scar tissue
These require nutritional correction first; stem cells help but aren’t primary treatment
Stem cells help but require dermatology co-management and immune-suppressing therapies
Realistic Expectations
If you’re a good candidate, here’s what to expect realistically:
- Hair density increase of 15–35% (not 100% regrowth of lost hair)
- Thicker, healthier-looking hair even if density increase is modest
- Stabilized hair loss (no further shedding acceleration)
- Results visible after 3–4 months, peak by 6–12 months
- Duration: 1–3+ years reported (varies individually; some patients may choose repeat treatments)
Individual results vary. Some patients see dramatic improvements. Others see modest but meaningful improvements. Genetics, age, and duration of hair loss all influence the outcome.
Hair regeneration without lifelong medication.
Stem cell therapy — from $19,800 USD per session
$19,800 USD includes:
- 100 million autologous ADSCs
- 7-week culture at MHLW-certified CPC · passage ≤3
- Quality certificate · 95%+ viability
- 1 / 3 / 6 month remote follow-up
Final pricing depends on your individual case:
- Higher cell counts (200 million+)
- Combination protocols
- Multiple sessions
Have Dr. Wakabayashi review your case.
Share your medical history and current treatments. Dr. Wakabayashi reviews each international inquiry and responds with a written feasibility note, recommended protocol, and quote. Typical turnaround: 1–3 business days.
Frequently Asked Questions
Does stem cell therapy for hair loss actually work?
A 2024 systematic review of 12 randomized controlled trials covering 514 patients confirmed statistically significant hair density and count increases across stem cell-derived therapies (multiple cell sources), with no serious adverse events reported. Gentile (2019) reported a 33% ± 7.5% hair density increase at 23 weeks, declining to 27% ± 3.5% at 44 weeks. A 2023 meta-analysis specifically of ADSC-derived conditioned media (8 trials, n=221) showed a pooled mean increase in hair density of approximately 14.93/cm² (p<0.0001). Individual results vary depending on hair loss stage, age, and genetics.
What is stem cell therapy for hair loss?
Stem cell therapy for hair loss is a non-surgical regenerative approach that uses a patient’s own adipose-derived stem cells (ADSCs) to support the biological environment of the scalp. Cells are harvested from abdominal fat, cultured for approximately seven weeks in a licensed laboratory, then injected into the scalp where they secrete growth factors that aim to support blood supply, follicle reactivation, and dermal papilla function.
What are the side effects of stem cell therapy for hair loss?
Published clinical trials report no serious adverse events across 514 patients in the 2024 systematic review of 12 RCTs. Temporary, expected effects include mild scalp redness, swelling, or tenderness at injection sites, typically resolving within 3–7 days. Because Cell Grand Clinic uses autologous (your own) cells, there is no risk of allogeneic immune rejection. No infections, scarring, or nerve injuries have been documented in the peer-reviewed trials we reference.
Can women with FAGA receive stem cell therapy for hair loss?
Yes. A 2025 controlled trial by Moneib et al. (n=33 women with Female Androgenetic Alopecia) showed improved hair density, thickness, and follicular unit numbers after autologous cultured ADSC scalp injection, with measurable changes in follistatin and DKK-1 signaling markers. Unlike finasteride, which is contraindicated in pregnancy, stem cell therapy does not interfere with hormone systems.
Stem cell therapy vs. hair transplant — which is better?
They solve different problems. Hair transplants move existing hair from a donor area to balding regions — permanent for transplanted hairs, but limited by donor follicle supply and typically $15,000–$50,000 per procedure. Stem cell therapy aims to support follicles across the scalp non-surgically, making it suitable for diffuse thinning and FAGA where transplants don’t apply. Some patients use both: transplant for established bald areas, stem cell therapy for density support in remaining follicles.
How long does stem cell hair therapy last?
Reported durability is 1–3+ years in published case series for autologous ADSC-related therapies, though individual results vary with age, genetics, and ongoing AGA/FAGA progression. Results are not permanent because hair loss itself is a progressive, genetic condition — but biological improvements in vascular support and dermal papilla activity can persist beyond a single treatment. Annual maintenance injections are recommended for long-term optimization.
Can stem cell therapy be combined with finasteride or minoxidil?
Yes — the mechanisms can be complementary. Finasteride suppresses DHT, while stem cell therapy aims to support the follicle environment. Minoxidil can extend the anagen phase while stem cells aim to support the surrounding tissue. Some patients use combination protocols, but combination decisions should be made with your physician based on your specific case and history.
Closing: Why Now?
Hair loss is progressive. The longer you wait, the more follicles miniaturize past the point of easy reactivation. A follicle that's been dormant for 2 years is easier to reawaken than one dormant for 10 years—and much easier to save before it becomes dormant at all.
If you're in early-to-moderate hair loss and considering stem cell therapy, the time to act is now. Not impulsively—but thoughtfully, with a consultation, with full information, with realistic expectations.
Finasteride and minoxidil are management tools. Hair transplant is a localized solution. Stem cell therapy is the only treatment that addresses the biological cause of hair loss—and it works non-surgically, without daily medication, for both men and women.
Reach us directly — WhatsApp and email inquiries are free of charge. Our English-speaking team will review your photos, assess your candidacy, and explain your options.
References
According to PubMed:
Legiawati, L., Sitohang, I. B. S., Yusharyahya, S. N., Sirait, S. P., Novianto, E., Liem, I. K., … Lauren, B. C. (2025). Hair regeneration in androgenetic alopecia using secretome of adipose-derived stem cells (ADSC) and minoxidil: a comparative study of three groups. Archives of Dermatological Research, 317(1), 486. DOI
Garza, L. A., Yang, C. C., Zhao, T., Blatt, H. B., Lee, M., He, H., … Cotsarelis, G. (2011). Bald scalp in men with androgenetic alopecia retains hair follicle stem cells but lacks CD200-rich and CD34-positive hair follicle progenitor cells. Journal of Clinical Investigation, 121(2), 613–622. DOI
Matsumura, H., Mohri, Y., Binh, N. T., Tateishi, T., Harada, M., Nakamura, Y., … Nishimura, E. K. (2016). Hair follicle aging is driven by transepidermal elimination of stem cells via COL17A1 proteolysis. Science, 351(6273), aad4395. DOI
Gentile, P. (2019). Autologous cellular method using micrografts of human adipose tissue derived follicle stem cells in androgenic alopecia. International Journal of Molecular Sciences, 20(14), 3446. DOI
Tak, Y. J., Lee, S. Y., Cho, A. R., & Kim, Y. S. (2020). A randomized, double-blind, vehicle-controlled clinical study of hair regeneration using adipose-derived stem cell constituent extract in androgenetic alopecia. Stem Cells Translational Medicine, 9(8), 839–849. DOI
Gasteratos, K., Kouzounis, K., & Goverman, J. (2024). Autologous stem cell-derived therapies for androgenetic alopecia: A systematic review of randomized control trials on efficacy, safety, and outcomes. Plastic and Reconstructive Surgery Global Open, 12(2), e5606. DOI
Moneib, H., Fathy, G., Samir, N. A., El-Khazragy, N., & El-Bassiouny, M. (2025). Successful treatment of female pattern hair loss with injection of autologous adipose-derived adult stem cells. International Journal of Trichology, 17(2), 113–120. DOI
Shin, H., Ryu, H. H., Kwon, O., Park, B. S., & Jo, S. J. (2015). Clinical use of conditioned media of adipose tissue-derived stem cells in female pattern hair loss: A retrospective case series study. International Journal of Dermatology, 54(6), 730–735. DOI
Yano, K., Brown, L. F., & Detmar, M. (2001). Control of hair growth and follicle size by VEGF-mediated angiogenesis. Journal of Clinical Investigation, 107(4), 409–417. DOI
Zuk, P. A., Zhu, M., Mizuno, H., Huang, J., Futrell, J. W., Katz, A. J., Benhaim, P., Lorenz, H. P., & Hedrick, M. H. (2001). Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Engineering, 7(2), 211–228. DOI
Chien, W. Y., Huang, H. M., Kang, Y. N., Chen, K. H., & Chen, C. (2023). Stem cell-derived conditioned medium for alopecia: A systematic review and meta-analysis. Journal of Plastic, Reconstructive & Aesthetic Surgery, 88, 182–192. DOI
Updated: 2026.06.06